
Table of Contents
What Are Sausage Eyes After Double Eyelid Surgery?
A sausage eye is the thick, puffy fold that can remain after double eyelid surgery, where the strip of skin between the crease and the lashes stays swollen and rounded instead of folding cleanly. It does not settle with time, and it is not slow healing. It comes from one of three structural causes: a crease fixed too high for your anatomy, an uncorrected ptosis that leaves the levator muscle too weak, or over-resection of the soft tissue. Which cause you have decides which revision will actually fix it. Choosing the wrong method in the first place is often what starts it, and our guide to incisional versus non-incisional double eyelid surgery explains which eyelid belongs to which technique.
This guide walks through each cause, how a surgeon tells them apart, why a loosening crease is a different problem, when to wait before revising, and the techniques used to correct each one.
The Complex Reality of Blepharoplasty Revision
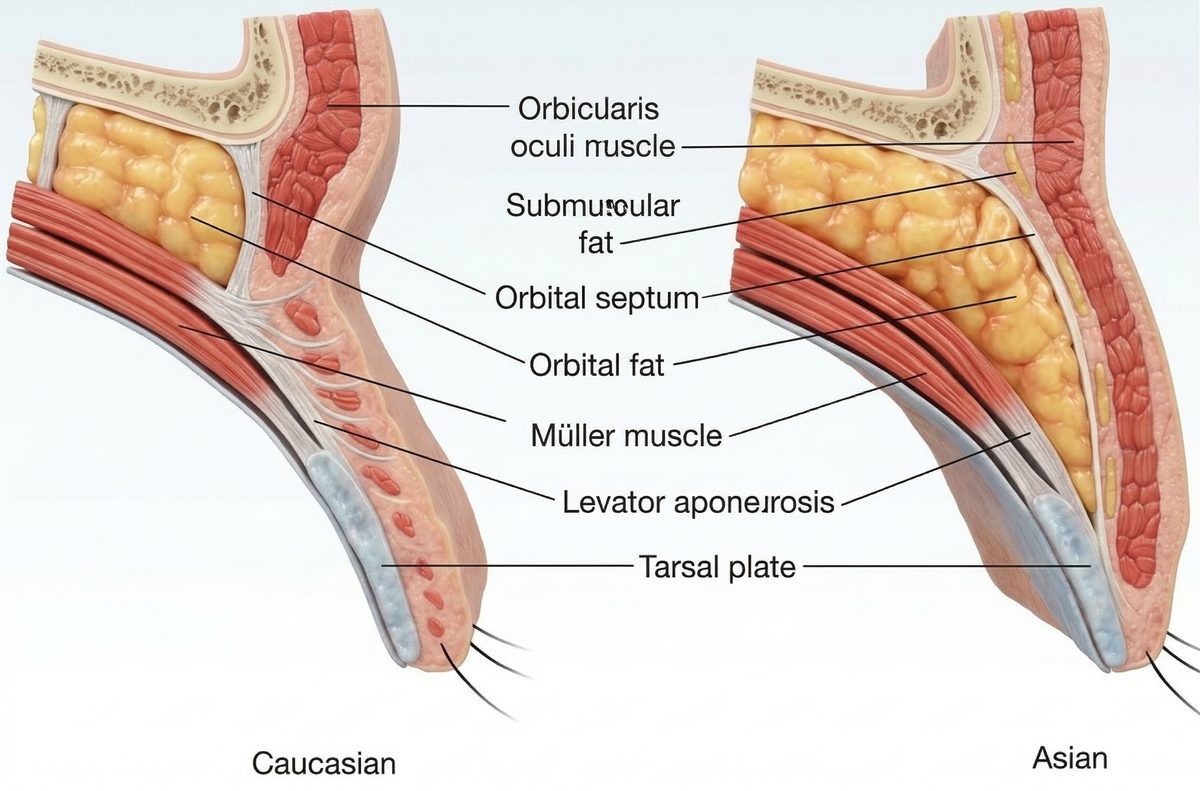
Double eyelid surgery — formally known as Asian blepharoplasty — remains one of the most frequently performed cosmetic procedures across East Asia and, increasingly, the world. Yet its popularity is accompanied by a significant and growing demand for double eyelid revision to correct outcomes that fall short of expectations. The persistently swollen, heavy fold known as a “sausage eye” and the gradual loosening and disappearance of the crease are the two most common reasons patients seek blepharoplasty revision. The operation itself may appear deceptively straightforward: a surgeon creates a supratarsal crease in the upper eyelid to produce the appearance of a defined double fold. Beneath that apparent simplicity, however, lies an intricate interplay of tissue layers — skin, orbicularis oculi muscle, orbital septum, preaponeurotic fat, levator aponeurosis, Müller’s muscle, and the tarsal plate — all compressed into a vertical span of barely fifteen millimeters.
It is precisely this anatomical density that explains why the procedure carries such a substantial revision rate. Double eyelid revision is not simply a matter of redrawing a line on the eyelid. It is a reconstructive undertaking that demands an entirely different surgical mindset. The revision surgeon must navigate through distorted tissue planes, dismantle fibrotic scar adhesions from the primary procedure, and address the precise mechanical failures that produced the unsatisfactory result. Without a thorough understanding of the anatomical origin of the problem, even a technically skilled reoperation risks repeating — or compounding — the original error.
For patients who have endured months or years of psychological distress, looking in the mirror and seeing an outcome that feels unrecognizable, grasping the “why” behind a failed result can itself be profoundly therapeutic. The sections that follow are intended to provide exactly that clarity — a detailed, anatomically grounded explanation of the two most common categories of double eyelid failure, and the reconstructive principles that guide their correction.
Decoding the 'Sausage Eye' (High Fold) Phenomenon
Among the most distressing outcomes a patient can face after double eyelid surgery is the so-called “sausage eye.” The term, though informal, captures the condition with uncomfortable accuracy: the segment of eyelid skin between the crease and the lash margin appears persistently swollen, heavy, and turgid, projecting outward in a rounded, sausage-like contour. This puffiness does not resolve with time. It persists months and even years after the initial operation, resistant to cold compresses, anti-inflammatory medication, and every home remedy patients desperately attempt.
Many patients are told — sometimes by the very surgeon who performed the original procedure — that they are simply “slow healers,” or that the swelling will eventually subside. In most cases, this reassurance is misguided. What appears to be chronic edema is, in fact, a structural anomaly rooted in one of three distinct anatomical errors, each of which alters the biomechanics of the eyelid in a different way.
1. Excessively High Fixation (The High Fold)
The single most prevalent cause of sausage eye is fixation of the double eyelid crease at a position that is too high relative to the patient’s native anatomy — the condition formally described as high fold blepharoplasty failure. To understand why this produces such a dramatic effect, it is helpful to consider the vertical architecture of the upper eyelid.
The tarsal plate — a dense, semirigid cartilaginous structure that provides the eyelid with its structural framework — typically measures between six and ten millimeters in height in East Asian patients. In a natural double eyelid, the supratarsal crease forms at or just above the superior border of this plate, roughly six to eight millimeters from the lash line. At this height, the overlying skin is thin, pliable, and relatively devoid of subcutaneous fat, allowing it to fold inward with elegant economy when the eye opens.
As one moves superiorly from the tarsal border toward the orbital rim, the tissue composition changes considerably. The skin thickens. The orbicularis oculi muscle gains volume. And critically, a layer of submuscular fat known as the retro-orbicularis oculi fat pad (ROOF) becomes increasingly prominent. When a surgeon anchors the crease into this thicker, heavier zone — whether from an overly ambitious aesthetic plan or a failure to account for the patient’s tissue characteristics — the fold does not tuck neatly inward. Instead, the dense, fat-laden skin beneath the crease buckles outward, producing the characteristic fullness.
But the problem extends beyond simple tissue mechanics. The upper eyelid relies on a delicate network of lymphatic and venous channels to drain interstitial fluid. These micro-vessels course through the preseptal tissue in a predominantly vertical orientation. A crease set too high effectively creates a horizontal dam across these drainage pathways, producing a state of chronic lymphatic stasis. Fluid that would normally be cleared within hours accumulates in the pretarsal segment, creating a boggy, waterlogged quality that no amount of elevation or massage can resolve. The result is a permanently puffy, distended fold — the hallmark sausage eye.
This is why sausage eye correction — one of the most sought-after double eyelid revision procedures in Korean plastic surgery — so frequently centers on the principle of line lowering: the crease must be repositioned to a height where the natural tissue anatomy permits both graceful folding and resolution of the chronic lymphatic stasis that sustains the puffiness.
2. Uncorrected Ptosis (Weak Levator Muscle)
Ptosis — the pathological drooping of the upper eyelid — is a condition of the levator aponeurosis, the thin but remarkably powerful tendinous expansion of the levator palpebrae superioris muscle that is responsible for elevating the eyelid. In its normal state, the levator aponeurosis inserts into the anterior surface of the tarsal plate and transmits the contractile force of the levator muscle, pulling the eyelid upward and exposing the pupil.
When the levator aponeurosis is attenuated, dehisced, or congenitally weak, the eyelid cannot open to its full excursion. The eye appears sleepy, the superior pupillary margin is partially obscured, and the patient unconsciously recruits the frontalis muscle to compensate, producing characteristic horizontal forehead creases.
Now consider what happens when a surgeon creates a double eyelid crease in a ptotic eye without simultaneously correcting the underlying levator dysfunction. The crease is designed to fold inward when the eye opens — but in a ptotic lid, the opening force is insufficient. The levator cannot generate enough upward traction to pull the skin fold deeply into the superior sulcus. Instead of tucking inward, the pretarsal skin remains partially prolapsed, bulging outward over the lash line. The visual effect is virtually indistinguishable from a high-fold sausage eye, though the underlying mechanism is entirely different.
This distinction carries profound implications for revision strategy. Lowering the crease height will not resolve a sausage eye caused by ptosis. The solution lies in ptosis correction — reinforcing or advancing the levator aponeurosis (or, in select cases, performing a Müller’s muscle–conjunctival resection) to restore adequate opening force. Only when the eye can open fully will the crease fold inward as intended, and the pretarsal puffiness dissipate.
3. Over-Resection of Soft Tissues
The third anatomical pathway to sausage eye formation involves excessive removal of the eyelid’s native soft tissues during the primary surgery. In the pursuit of a “clean” or “defined” crease, some surgeons aggressively excise preaponeurotic orbital fat, ROOF fat, or segments of the orbicularis oculi muscle. While conservative sculpting of these tissues can be entirely appropriate, over-resection triggers a cascade of complications that are exceptionally difficult to reverse.
The orbital fat pads and orbicularis muscle serve a critical biomechanical role that extends beyond mere volume. They function as a gliding interface — a lubricated tissue plane that allows the skin to move independently over the deeper levator aponeurosis and tarsal plate during blinking and eye opening. When this gliding layer is removed, the overlying skin loses its independent mobility. It adheres directly to the rigid deeper structures through fibrotic scarring, creating a tethered, concave indentation at the crease line.
The consequences are twofold. First, the indented crease restricts the natural excursion of the eyelid skin, limiting the smooth upward folding that defines a graceful double eyelid. Second, the remaining tissue above and below the tethered scar, deprived of its natural support and redistribution mechanism, bulges outward under the influence of gravity and muscular contraction. The result is a deeply grooved, irregular fold with pronounced adjacent fullness — a particularly severe and cosmetically distressing variant of the sausage eye.
Sausage eye correction for this variant demands not only scar release but also volume restoration. Autologous fat grafting, orbital fat repositioning, or the interposition of vascularized tissue flaps may be required to reconstitute the lost gliding plane and restore the eyelid’s natural biomechanical fluidity.
Why Do Double Eyelids Unfold? The Mechanics of Loosening

At the opposite pole of the complication spectrum lies a problem that is no less frustrating for the patient: double eyelid loosening — the gradual attenuation and eventual disappearance of the fold. Where the sausage eye represents an excessively robust, albeit misdirected, adhesion, loosening reflects the failure of the surgical adhesion to withstand the repetitive biomechanical forces that act upon the eyelid thousands of times each day with every blink. For patients experiencing double eyelid loosening, understanding the mechanical cause is the essential first step toward planning an effective revision.
A durable double eyelid fold depends on the formation of a stable fibrous connection between the dermis of the eyelid skin and the underlying levator aponeurosis or tarsal plate. This connection must be strong enough to reproduce the natural crease-forming mechanism found in eyelids that possess a congenital double fold, where fibers from the levator aponeurosis naturally extend through the orbicularis muscle to insert into the dermal layer of the skin. When this surgically created adhesion is mechanically inadequate, it gradually attenuates and ultimately fails, allowing the fold to unfurl.
Two primary factors account for the vast majority of loosening cases:
Inadequate Method for Skin Thickness and Volume. The non-incisional (suture-based) technique for double eyelid creation has earned widespread popularity owing to its minimal downtime, absence of a visible scar, and reversibility. In carefully selected patients — those with thin eyelid skin, minimal orbicularis hypertrophy, and scant ROOF fat — it produces elegant, lasting results.
However, when this technique is applied to patients whose tissue characteristics fall outside its ideal parameters, the outcome is predictably temporary. Thick, sebaceous skin exerts greater gravitational load on the suture points. A voluminous orbicularis muscle resists the infolding required to maintain the crease. And an abundant ROOF fat pad cushions and insulates the suture from forming a firm dermal–aponeurotic adhesion.
Over weeks or months, the tissue memory of these dense structures gradually overpowers the mechanical hold of the buried sutures. The adhesion stretches, the crease becomes shallow, and eventually the fold vanishes entirely — often asymmetrically, adding to the patient’s distress. In such patients, the incisional technique, which permits direct visualization, controlled tissue removal, and a more robust dermal fixation, is the anatomically sound choice.
Tension from the Epicanthal Fold (Mongolian Fold). The epicanthal fold — a crescent of skin that drapes over the medial canthus (inner corner) of the eye — is a defining anatomical feature in many East Asian eyelids. While often regarded as a purely aesthetic characteristic, it exerts a powerful and frequently underestimated mechanical influence on the double eyelid crease. The epicanthal fold generates a persistent vector of tension directed medially and inferiorly, pulling the nasal portion of the crease downward and inward toward the inner canthus.
If a surgeon designs an in-fold (tapering) or parallel crease configuration without first addressing this opposing force — typically through an epicanthoplasty or medial canthoplasty to release the epicanthal tension — the crease finds itself in a state of constant biomechanical conflict. The surgical adhesion is continuously stressed by the epicanthal fold’s pull, and over time, this unrelenting tension overcomes the fixation.
The crease begins to loosen from the medial aspect, propagating laterally until the fold is significantly diminished or entirely lost. This mechanism explains why so many patients experiencing double eyelid loosening report that their fold “disappeared from the inner corner first” — a clinical observation that is entirely consistent with the directional force exerted by the epicanthal fold.
The Surgeon’s Approach: Double Eyelid Revision Techniques
Revising a failed double eyelid is a fundamentally different surgical endeavor from performing a primary blepharoplasty. The tissue planes have been disrupted. Scar tissue has formed in unpredictable configurations. The blood supply may be compromised by prior dissection. And the patient’s psychological investment in the outcome is, understandably, far greater. A board-certified Korean plastic surgery specialist approaches double eyelid revision not by imposing a new aesthetic template, but by diagnosing the specific structural failure — whether it stems from high fold blepharoplasty, uncorrected ptosis, or tissue over-resection — and restoring the anatomical conditions necessary for a stable, natural-appearing fold.
Scar Release and Line Lowering (“Two-Line” Technique)
For patients whose sausage eye stems from an excessively high fixation, the cornerstone of correction is the “two-line” or line-lowering technique — a procedure that is as conceptually elegant as it is technically demanding.
The surgeon begins by meticulously identifying the existing high crease and mapping the desired new crease at an anatomically appropriate height, typically aligned with the superior border of the tarsal plate. Through a carefully planned incision at the new, lower position, the surgeon performs a precise subcutaneous and sub-orbicularis dissection to reach the fibrotic adhesion band of the original crease. This scar tissue — often remarkably dense and tenacious after months or years of maturation — must be completely released. Incomplete lysis of the old adhesion is one of the most common causes of persistent sausage eye after revision, as even a residual band of scar can re-tether the skin and recreate the original deformity.
Once the restrictive adhesion has been fully liberated, the surgeon faces a critical reconstructive challenge: preventing the released tissues from simply re-scarring back to the old, high crease line. This is accomplished by interposing a biological barrier between the freed skin flap and the deeper structures at the original fixation site. Depending on the patient’s anatomy and the degree of tissue deficiency, this barrier may take the form of repositioned preaponeurotic orbital fat, a pedicled ROOF fat flap, or, in cases of significant volume depletion, autologous fat grafting. The interposed tissue serves a dual purpose — it physically blocks re-adhesion at the old height while simultaneously restoring the gliding layer that permits smooth eyelid mechanics.
A new fixation is then established at the lower crease position, anchoring the dermis to the levator aponeurosis at the desired height with meticulous attention to symmetry, depth, and tension. The result, when executed with precision, is a dramatic transformation: the pretarsal puffiness resolves, the eyelid contour softens, and the crease assumes a natural, proportionate position.
Dynamic Ptosis Correction
When uncorrected ptosis is identified as a contributing or primary factor in the failed result, ptosis correction becomes an indispensable component of the revision surgery — not an optional addendum. The biomechanical logic is straightforward: no crease design, however anatomically perfect in its height and fixation, can fold inward properly if the levator muscle lacks the contractile force to pull it into the sulcus.
The specific ptosis correction technique is tailored to the severity of the dysfunction and the condition of the levator complex. In cases of aponeurotic ptosis — the most common etiology in the revision population — the levator aponeurosis is identified, advanced, and resecured to the anterior surface of the tarsal plate, effectively shortening its excursion and amplifying the mechanical opening force. For milder degrees of ptosis, a Müller’s muscle–conjunctival resection (posterior approach) may be appropriate, offering the advantage of avoiding additional anterior dissection in already-scarred tissue planes.
The functional and aesthetic benefits of ptosis correction extend beyond resolving the sausage eye phenomenon. By increasing the opening excursion of the eyelid, the procedure enhances the visible exposure of the pupil and the superior iris, producing a brighter, more alert, and more youthful appearance. The crease, now backed by adequate levator force, tucks inward crisply with each eye opening — a dynamic result that static scar adhesion alone can never replicate.
The Golden Time for Blepharoplasty Revision
Patience is not merely a virtue in the double eyelid revision journey — it is a clinical imperative. The universally accepted standard is to wait a minimum of six months after the primary Asian blepharoplasty before undertaking a secondary procedure, and in many cases, a full twelve months is preferable.
The rationale for this waiting period is grounded in the biology of wound healing. During the first several months after surgery, the eyelid tissues exist in a state of active remodeling. Collagen fibers are being deposited, cross-linked, and reorganized. The scar tissue is indurated — firm, edematous, and inflamed. Blood supply to the operative field is in the process of reconstituting through neovascularization. The true anatomical landmarks — the position of the crease, the degree of adhesion, the extent of tissue deficiency — are obscured by this biological turbulence.
Operating during this volatile phase carries substantial risks. Inflamed, friable tissues do not hold sutures reliably. Edematous tissue planes are difficult to identify and dissect cleanly. And the active scarring process means that even a technically perfect revision can be undermined by unpredictable postoperative fibrosis, potentially creating a result worse than the one the patient sought to correct.
By waiting for the scar to mature and soften — a process that follows a well-characterized biological timeline — the revision surgeon gains several critical advantages: the tissue planes become identifiable, the scar tissue can be precisely delineated and released, the blood supply has stabilized, and the patient’s anatomy can be assessed in its true, settled state. This patience, though difficult for patients understandably eager for resolution, is one of the most important factors in achieving a successful revision outcome.
Why Blepharoplasty Revision Demands Specialized Expertise
The upper eyelid is a marvel of anatomical engineering — a structure barely a millimeter thick in places, yet composed of multiple dynamic layers of skin, muscle, connective tissue, fat, and fascia, all working in concert to perform the essential functions of blinking, eye protection, and tear distribution. Within this exquisitely compact architecture, even a one-millimeter miscalculation in crease height, a slight imbalance in tissue resection, or a subtle failure to identify underlying ptosis can translate into a visibly unnatural result.
Revision surgery compounds these challenges exponentially. The tissue planes have been violated. Scar has formed where native tissue once existed. The blood supply has been altered. The margin for error, already narrow in primary surgery, becomes vanishingly thin.
This is why blepharoplasty revision in South Korea — where Korean plastic surgery specialists perform a higher volume of double eyelid revision procedures than perhaps anywhere else on earth — has evolved into a distinct subspecialty, demanding a level of anatomical knowledge, surgical precision, and clinical judgment that exceeds the requirements of primary blepharoplasty by a considerable margin. Patients seeking double eyelid revision to resolve sausage eyes, loosening folds, or any other complication of prior eyelid surgery must prioritize one criterion above all others: a board-certified plastic surgeon with deep, specialized expertise in both aesthetic and reconstructive periocular surgery.
True correction lies not in simply operating again, but in understanding why the first operation failed — and in possessing the anatomical fluency and technical mastery to address the root cause. In plastic surgery, lasting beauty is always built on a foundation of sound anatomy.
Surgeon’s Insight: The most successful double eyelid revision is one that leaves no trace of having been revised at all. When a patient opens their eyes and the fold tucks inward with effortless precision — no puffiness, no tethering, no asymmetry — that is the moment you know the anatomy has been truly restored, not merely rearranged. Every sausage eye and every loosened crease tells a specific anatomical story; the surgeon’s task is to read that story accurately before picking up a scalpel. Rushing to operate without understanding the structural failure is the single most common reason revisions fail a second time.
Considering a broader facial rejuvenation? Learn how lower eyelid concerns differ from upper lid revision in our guide to lower blepharoplasty vs. tear trough fillers.
Written by Dr. Yongwoo Lee, board-certified plastic surgeon specializing in blepharoplasty and anti-aging surgery at VIP Plastic Surgery, South Korea.
Frequently Asked Questions About Double Eyelid Revision
What are sausage eyes after double eyelid surgery?
A sausage eye is a fold that stays thick, puffy, and rounded instead of folding cleanly, and it does not settle with time. It comes from a crease fixed too high, an uncorrected ptosis, or over-resection of tissue. Because the three causes need different operations, an accurate diagnosis matters more than the revision technique itself.
How long should I wait before getting a double eyelid revision?
The standard recommendation is to wait at least six months after the initial surgery, though many experienced revision surgeons prefer to wait a full year for optimal tissue maturation. During this period, the scar tissue from the primary procedure undergoes active remodeling — it is initially firm, inflamed, and unpredictable, gradually softening and stabilizing over time. Attempting a revision while the tissues are still in this volatile healing phase significantly increases the risk of unpredictable scarring, poor tissue handling, and a compromised final result. The waiting period allows the anatomy to settle into its true, definitive state, enabling the surgeon to make an accurate diagnosis and execute precise, controlled corrections.
Can a “sausage eye” (high fold) be completely fixed?
Yes, in the majority of cases, sausage eye correction can be achieved successfully and comprehensively. The most widely employed technique is the “two-line” or line-lowering procedure, in which a board-certified plastic surgeon carefully releases the fibrotic adhesion at the original, excessively high crease and establishes a new fold at an anatomically appropriate lower position. To prevent recurrence, orbital fat or vascularized tissue flaps are typically interposed as a biological barrier, blocking the released tissues from re-scarring to the old crease line. When ptosis is identified as a contributing factor, simultaneous levator advancement or repair is performed to ensure adequate eyelid opening force. The combined result is a natural, unswollen eyelid contour with a proportionate, well-defined crease.
Will my eyes look natural after a blepharoplasty revision?
Achieving a natural appearance is the fundamental objective of every revision procedure, and in skilled hands, it is a realistic expectation. However, it is important to understand that revision surgery is inherently more complex than primary blepharoplasty. The surgeon must work within tissue planes that have been previously disrupted, navigate existing scar formations, and contend with potentially altered blood supply. Success depends not on simply adjusting the visible crease line, but on diagnosing and correcting the specific underlying structural failure — whether that is an excessively high fixation, uncorrected ptosis, over-resected tissues, or epicanthal fold tension. The selection of a highly experienced, board-certified plastic surgeon who specializes in revisional periocular surgery remains the single most important factor in achieving the most natural-looking outcome.
What is the difference between sausage eye from a high fold and sausage eye from ptosis?
Although both conditions produce a visually similar appearance — a persistently puffy, swollen pretarsal segment — their anatomical origins and treatment strategies differ substantially. A sausage eye caused by an excessively high fold results from the crease being anchored above the natural tarsal plate boundary, forcing thick, fat-laden skin to buckle outward and obstructing lymphatic drainage. Correction involves lowering the crease height. A sausage eye caused by uncorrected ptosis, on the other hand, results from insufficient levator muscle force: the eyelid cannot open fully, so the skin fails to tuck inward at the crease. Correction requires strengthening or advancing the levator aponeurosis. An accurate differential diagnosis between these two mechanisms is essential, as applying the wrong correction will fail to resolve — and may worsen — the deformity.
Can the non-incisional (suture) method be used for revision surgery?
In most revision scenarios, the non-incisional suture technique is not recommended. Revision surgery typically requires direct access to the tissue planes for scar release, tissue repositioning, and secure fixation — objectives that cannot be reliably achieved through buried sutures alone. The incisional approach provides the surgeon with full visualization of the altered anatomy, precise control over scar dissection and tissue manipulation, and the ability to create a more robust dermal–aponeurotic adhesion. For the correction of sausage eyes, significant loosening, or structural failures, the incisional method is the standard of care.
Why is blepharoplasty revision considered more difficult than primary surgery?
Revision surgery is inherently more challenging because the surgeon must operate within an anatomical landscape that has been fundamentally altered by the primary procedure. Native tissue planes have been disrupted and replaced by scar. Soft tissue volume may have been reduced by prior resection. The blood supply has been compromised by previous dissection. And the biomechanical relationships between the skin, muscle, and deeper structures may have been changed in ways that are not immediately apparent on external examination. These factors demand a higher level of anatomical knowledge, more refined surgical judgment, and greater technical precision than a primary procedure — which is why patients are strongly advised to seek a board-certified plastic surgeon with specific expertise in revisional eyelid surgery.
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified medical professional before making any decisions about surgical or non-surgical procedures.