Table of Contents
The Question That Splits Every Consultation in Two
If you are considering lower blepharoplasty to address under-eye bags, the choice between fat repositioning and fat removal is the single surgical decision that will determine how your eyes look not just next month, but ten and twenty years from now.
This is not an abstract academic debate. It is the clinical crossroads where lasting, natural rejuvenation separates from a hollowed, skeletonized appearance that can age your face faster than the original problem. Yet most patients walking into a consultation have never heard the distinction explained. You may have been told simply that the “bags will be taken away,” without any discussion of where the fat actually goes, or what happens to your lower eyelid contour five years later when the surrounding facial volume continues to diminish with age.
This article walks you through the anatomy of why fat repositioning produces a result that ages gracefully, why aggressive fat removal creates the dreaded hollow eyes after blepharoplasty, and how your surgeon evaluates your anatomy to determine the precise technique your face requires.
The Anatomy of Under-Eye Bags: Three Fat Compartments You Should Understand
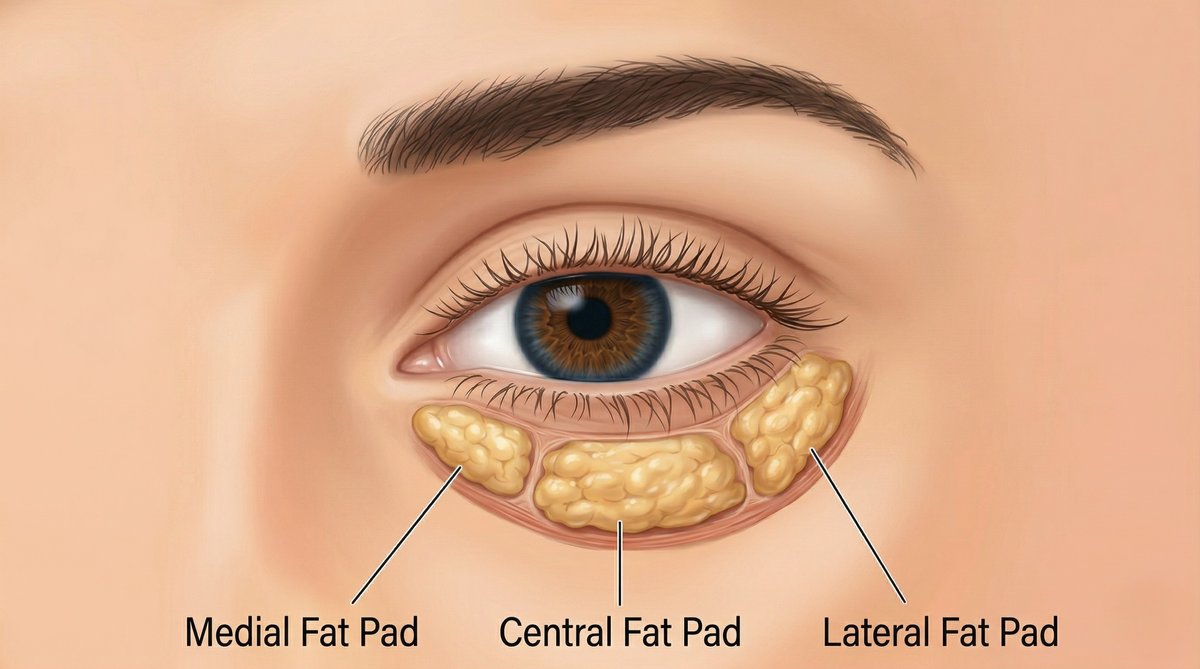
Your under-eye bags are not a single, homogeneous mass of tissue. The orbital fat that bulges forward beneath your lower eyelid is organized into three anatomically distinct compartments: the medial fat pad (closest to your nose), the central fat pad, and the lateral fat pad (closest to your temple).
Each compartment is separated by fascial septa and has a different relationship to the surrounding structures. The medial fat pad, for example, sits adjacent to the inferior oblique muscle, a critical structure that controls your eye movement. The central fat pad is the largest and most visually prominent when it herniates. The lateral fat pad is the smallest and often contributes to subtle fullness that blends into the cheek.
What creates the visible “bag” beneath your eye is not actually excess fat in most cases. It is the forward herniation of normal orbital fat through a weakened orbital septum. The septum, a thin fibrous membrane that holds the fat behind the orbital rim, thins and loosens with age. Once the structural containment weakens, gravity and orbital pressure push the fat pads forward, creating the characteristic convex bulging that makes you look exhausted regardless of how well you slept.
Directly below these bulging fat pads lies the tear trough, the concave groove that runs from the inner corner of your eye along the orbital rim toward the cheek. In a youthful face, there is a smooth, continuous convexity from the lower eyelid to the cheek. In an aging face, the contrast between the bulging fat above and the hollow trough below creates a shadow that is responsible for most of the “tired” appearance you see in the mirror.
Fat Removal: The Subtractive Approach and Its Long-Term Cost
Traditional lower blepharoplasty, as it was practiced for decades, treated under-eye bags as a straightforward volume problem. The logic was simple: there is too much fat, so remove it. The surgeon would open the orbital septum, identify the herniated fat pads, excise them, and close. The immediate result was often dramatic. The bags vanished, and the lower eyelid appeared smooth and flat.
The problem only reveals itself over time.
Your face does not stop aging on the day of surgery. In the years following a fat removal blepharoplasty, the remaining orbital fat continues to atrophy naturally. The midface volume continues to deflate. The cheek pad descends. The bone remodels. Every one of these age-related changes deepens the very hollow that aggressive fat excision created, and the result is a progressive sunken, skeletonized appearance around the eyes that is almost impossible to fully reverse.
This is the clinical entity known as hollow eyes after blepharoplasty, and it is one of the most frequently cited complications in the lower blepharoplasty literature. The eyes appear deep-set, dark, and cadaveric. The transition from the lower eyelid to the cheek, which should be a smooth youthful curve, instead collapses into a visible step-off. The A-frame deformity, where the lower orbital rim becomes skeletally visible, gives the face a gaunt, aged quality that is far worse than the original under-eye bags.
The critical insight is this: the fat you were born with is not the enemy. It is a structural asset. Removing it eliminates an immediate cosmetic concern at the expense of your long-term facial architecture.
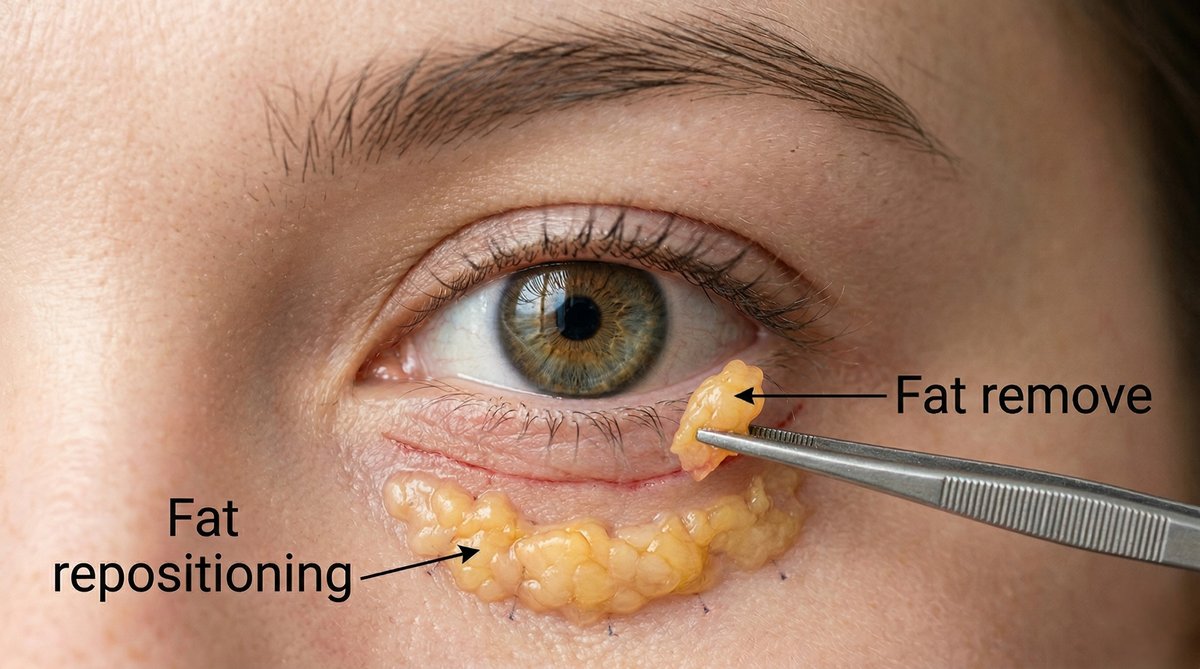
Fat Repositioning: Solving Two Problems with One Tissue
Fat repositioning represents a fundamental philosophical shift in lower blepharoplasty. Rather than discarding the herniated orbital fat, the surgeon releases it from its compartments, mobilizes it inferiorly over the orbital rim, and secures it into the tear trough depression. The fat that was creating a convex bulge above the rim is transposed to fill the concave hollow below it.
The elegance of this approach is that it solves two problems with a single tissue. The bag disappears because the fat has been relocated, and the tear trough fills because the fat now occupies the very space that was causing the hollow shadow. The transition from lower eyelid to cheek becomes the smooth, continuous convexity that defines a youthful periorbital contour.
Because no volume has been subtracted from the orbit, the result ages naturally alongside the rest of your face. As the surrounding tissues continue to lose volume over the decades, you are not starting from a deficit. The repositioned fat maintains structural support in the tear trough, preserving a smooth lid-cheek junction that fat removal cannot achieve.
How the Procedure Works
Through a transconjunctival approach, the surgeon accesses the orbital fat from the inside of the lower eyelid, leaving no visible scar on your skin. The herniated fat pads are carefully dissected free from the surrounding septa while preserving the inferior oblique muscle and the capsulopalpebral fascia. The mobilized fat is then draped over the arcus marginalis, the periosteal attachment along the inferior orbital rim, and sutured into position in the subperiosteal or supraperiosteal plane of the tear trough.
The technical precision required is significant. Each of the three fat compartments may contribute differently to your specific deformity, and the surgeon must assess in real time how much fat to transpose, at what vector, and how far inferiorly to extend the repositioning. Overcorrection creates an unnatural fullness below the rim. Undercorrection leaves a residual shadow. The target is a seamless, gradient transition from the lower eyelid to the midface.
When Fat Removal Is Still Appropriate
Fat repositioning is not universally superior in every clinical scenario. There are specific anatomical presentations where limited, conservative fat excision remains a valid component of the surgical plan.
If you present with genuinely excessive orbital fat volume, particularly in the medial compartment, repositioning the entire volume into the tear trough would create an overcorrected, puffy appearance below the orbital rim. In these cases, the surgeon may excise a measured portion of the medial fat while repositioning the central and lateral compartments. The key word is conservative: small, precise amounts are removed only when the total volume exceeds what the tear trough can physiologically accommodate.
Patients with a naturally full midface and minimal tear trough depression may also benefit from a hybrid approach. If there is no significant hollow to fill, transposing large volumes of fat into an already well-supported area creates an unnatural convexity.
The critical distinction is between a surgeon who removes fat because it is the only technique they offer, and a surgeon who selectively removes fat as part of a volume-preserving strategy that prioritizes your long-term contour. These are fundamentally different clinical philosophies, and the outcomes they produce diverge dramatically over time.
Surgeon’s Insight: The Principle of Dynamic Aesthetics
A lower blepharoplasty cannot be evaluated by examining the eye in isolation. The true test of a successful result is how the periorbital region integrates with the rest of your face during natural expression. This principle defines what experienced aesthetic surgeons refer to as Dynamic Aesthetics: the repositioned fat must create a contour that moves fluidly with your orbicularis oculi during smiling, squinting, and every microexpression in between.
During your procedure, the surgeon assesses the fat transposition not only with the face at rest but also with the lower eyelid under dynamic tension. You will be asked to look upward, downward, and laterally while the fat position is evaluated. The objective is not merely eliminating a bag but sculpting a lid-cheek junction that remains natural across the full range of your facial animation. When you smile and the orbicularis oculi contracts, the transition from eyelid to cheek should be seamless. That is the standard a board-certified plastic surgeon holds: not beauty at rest, but beauty in motion.

The Complication No One Warns You About: Lower Eyelid Retraction
Beyond hollow eyes, there is another complication that deserves your attention before choosing a surgeon. Lower eyelid retraction, where the lower lid margin is pulled downward to expose excessive scleral show beneath the iris, is a potentially devastating outcome that can follow any lower blepharoplasty but is more frequently associated with aggressive surgical techniques.
Retraction occurs when the delicate lamellae of the lower eyelid, the anterior skin-muscle layer and the posterior conjunctiva-tarsus layer, are disrupted, scarred, or shortened during surgery. Excessive cautery, aggressive skin removal, and failure to support the lateral canthus can all contribute. The result is a visible white crescent of sclera below your iris, a rounded or pulled-down lower lid contour, and in severe cases, frank ectropion with chronic dry eye symptoms.
The transconjunctival approach with fat repositioning inherently minimizes this risk. Because the incision is made on the inner surface of the eyelid and no skin is removed, the anterior lamella remains completely intact. The structural support of the lower lid is preserved, and the risk of retraction is substantially lower compared to transcutaneous approaches that involve skin-muscle flap dissection.
If your preoperative evaluation reveals any degree of lid laxity, horizontal lid shortening, or a negative canthal tilt, your surgeon should address these findings proactively with adjunctive canthopexy or canthoplasty to reinforce the lateral canthal tendon before the retraction risk materializes postoperatively.
Choosing Your Surgeon: The Questions That Matter
When you sit down for a lower blepharoplasty consultation, the answers to a few specific questions will tell you everything you need to know about the surgeon’s philosophy and your likely outcome.
Ask whether the plan involves fat removal, fat repositioning, or a combination. If the answer is fat removal alone with no mention of the tear trough, that is a signal to seek another opinion. Ask to see long-term results, not just one-week postoperative photographs, but images taken one, three, and five years after surgery. The short-term result of fat removal can look excellent. The long-term result often does not.
Ask about the surgical approach. The transconjunctival route with no external incision is the standard for most candidates, particularly if you have minimal skin excess. Ask whether canthal support will be assessed preoperatively. A thorough evaluation of your lid laxity, snap-back test, and distraction test demonstrates that the surgeon is thinking about the structural integrity of your eyelid, not just the fat.
In Korean plastic surgery, where anatomical precision and conservative technique define the standard of care, lower blepharoplasty has evolved into a volume-preserving procedure by default. The goal is not to subtract from your face but to redistribute what nature provided into a more harmonious configuration.
Considering how this philosophy applies to other facial concerns? Learn about the differences between tear trough fillers and lower blepharoplasty and why the temporary fix often cannot match the structural correction. For patients exploring upper eyelid surgery, understanding the anatomy of double eyelid revision offers another perspective on how precision determines outcomes in periorbital surgery.
Written by Dr. Yongwoo Lee, board-certified Korean plastic surgery specialist in facial anatomy and aesthetic procedures at VIP Plastic Surgery, South Korea.
Frequently Asked Questions About Fat Repositioning in Lower Blepharoplasty
What is fat repositioning in lower blepharoplasty?
Fat repositioning is a surgical technique where the herniated orbital fat that creates your under-eye bag is not removed but instead released, mobilized, and transposed over the inferior orbital rim into the tear trough depression. This simultaneously eliminates the visible bag and fills the hollow groove beneath it, creating a smooth transition from your lower eyelid to the cheek. Because no volume is subtracted, the result preserves your facial architecture and ages more naturally than techniques that rely on fat excision alone.
What causes hollow eyes after blepharoplasty?
Hollow eyes after blepharoplasty result from excessive removal of orbital fat during surgery. In the immediate postoperative period, the lower eyelid may appear smooth and rejuvenated. However, as your face continues to age and the surrounding tissues lose volume naturally, the orbital area that was stripped of its fat becomes progressively more sunken. The inferior orbital rim becomes skeletally visible, creating a deep shadow and a gaunt, cadaveric appearance. This complication is most common when all three fat compartments are aggressively excised without consideration for long-term volume loss.
Is fat repositioning better than fat removal for under-eye bags?
For the majority of patients, fat repositioning produces a superior long-term result. It treats both the bag and the tear trough hollow with a single tissue, preserves your native orbital volume, and creates a contour that ages alongside the rest of your face rather than collapsing over time. Fat removal may be appropriate in limited, specific cases where the total fat volume genuinely exceeds what the tear trough can accommodate, but even then, most experienced surgeons combine conservative excision with repositioning rather than relying on removal alone.
Does fat repositioning leave a visible scar?
When performed through the transconjunctival approach, fat repositioning leaves no visible scar on your skin. The incision is made on the inner surface of the lower eyelid, through the conjunctiva, and heals without any external evidence of surgery. This is the preferred approach for patients without significant lower eyelid skin excess. If you do have redundant skin that requires tightening, a small skin pinch excision can be added just below the lash line, leaving a nearly imperceptible scar that fades into the natural crease.
How long does recovery take after fat repositioning blepharoplasty?
Most patients experience noticeable bruising and swelling for seven to ten days following surgery. You can typically return to work and social activities within one to two weeks. The lower eyelid contour continues to refine over the following two to three months as residual edema resolves and the repositioned fat settles into its final position. Strenuous exercise and heavy lifting should be avoided for approximately three to four weeks to minimize the risk of postoperative bleeding or swelling. Your surgeon will provide a detailed recovery timeline specific to the extent of your procedure.
Can hollow eyes from a previous blepharoplasty be corrected?
Yes, although correction of hollow eyes after a previous fat removal blepharoplasty is more complex than a primary procedure. The most common approach involves volume restoration using autologous fat grafting, where fat harvested from another area of your body is carefully injected into the hollowed tear trough and orbital rim region. In some cases, dermal fillers can provide temporary improvement, but structural fat grafting offers a more permanent solution. The revision requires meticulous technique because the scar tissue from the original surgery alters the tissue planes and limits the predictability of fat graft survival.
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified medical professional before making any decisions about surgical or non-surgical procedures.