
Table of Contents
The Question Behind Every Eyelid Surgery Consultation
Sub-brow lift and upper blepharoplasty are the two operations most often discussed for heavy, hooded Asian upper eyelids, whether you have a monolid, a natural double eyelid, or a surgically created crease from a previous procedure. Both promise a lighter, more youthful eye. Both have decades of refinement behind them. Both, in the right hands, deliver beautiful results. And yet the right surgery for one patient is the wrong surgery for the next, even when their before-photos look nearly identical.
If you have searched for sub-brow lift, sub-brow blepharoplasty, or upper blepharoplasty, you have probably encountered conflicting recommendations. One clinic told you upper blepharoplasty. Another suggested sub-brow lift. A friend who looked great after one surgery swore by it, and then a different friend warned you off the same operation. That disagreement is not random. It reflects a fact most marketing language obscures: this decision is case-specific, governed by your anatomy, your existing eyelid type, and what you want your eye to look like after surgery.
This guide is built around that decision. It walks you through the two surgeries briefly, then maps eight common patient profiles to the correct procedure for each. By the end, you should be able to identify which case most closely resembles yours and which of the two operations matches your anatomy.
The Real Question You Should Be Asking
Most patients arrive at consultation asking “which surgery is better?” That question has no useful answer, because neither operation is universally better than the other. They address the same complaint, a heavy upper eyelid, from opposite ends of the lid-brow complex. Asking which is better is like asking whether a hammer is better than a screwdriver.
A useful question is anatomical and personal. Two specific variables determine which surgery fits you.
Variable one: where your excess tissue actually lives. Some patients carry their heaviness in the lid skin between the crease and the lash line. Others carry it in the thick sub-brow tissue just beneath the eyebrow itself. Many carry it in both zones, and the proportion between the two changes everything about the surgical plan.
Variable two: what you want your eye to look like afterward. If you have a monolid and want to keep your monolid identity, the right operation must not create a crease. If you have a soft natural crease and want to preserve its subtle character, the right operation must not deepen or sharpen it. If your existing surgical crease has faded and you want it sharper, that goal points in a different direction entirely.
These two variables are independent. You can be a monolid patient with heavy sub-brow tissue, or a double-eyelid patient with heavy lid skin, or any other combination. The eight patient profiles in the case-by-case section below cover the configurations seen most often in Korean plastic surgery practice.
A Quick Anatomy Primer
Your upper eyelid is not one tissue layer. Functionally, it works as two zones stacked together, each behaving differently with age, and the anatomy of the Asian upper eyelid makes that distinction unusually sharp.
The lid zone runs from your lash line up to the natural fold of your crease. Skin here is thin, mobile, and dynamically tied to the levator muscle that opens your eye. When excess tissue accumulates in this zone, you see a heavy fold sitting directly on your lashes, an effaced crease, or a stretched pretarsal band.
The sub-brow zone sits between your crease and the lower edge of your eyebrow. Skin here is notably thicker, especially in Asian patients, and it is anchored more to your brow than to your lid. When excess tissue accumulates in this zone, you see weight pressing down on your fold from above, lateral hooding above your outer corner, and a brow that appears to have descended toward the orbital rim.
These two zones age separately. Patients in their thirties often show change confined to one zone. Patients in their fifties usually show change in both, but in different proportions. Upper blepharoplasty addresses the lid zone. Sub-brow lift addresses the sub-brow zone. That is the entire foundation of the decision.
One more anatomical pattern matters. Aging in the Asian upper eyelid involves brow descent more than Caucasian aging does, because Asian brows sit lower against the supraorbital rim to begin with. When your brow descends, weight transfers into the sub-brow zone first and into the lid zone only secondarily. Recognizing this pattern is the difference between treating the symptom and treating the source.
How the Two Surgeries Actually Differ
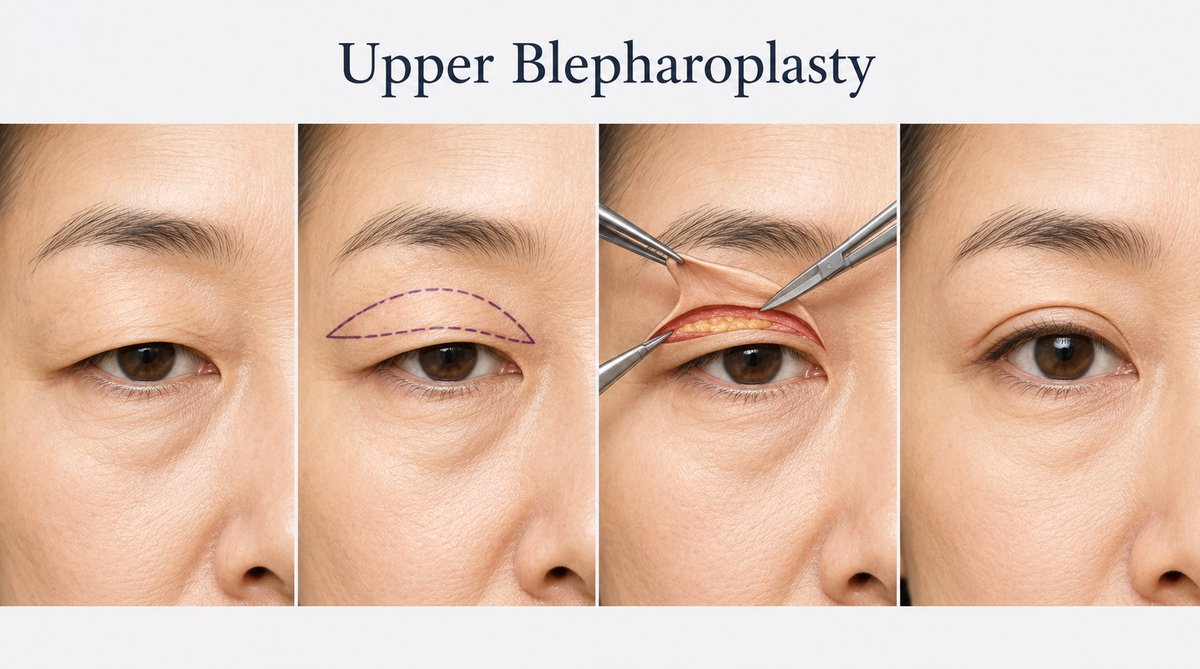
Upper blepharoplasty removes a strip of skin from the lid zone. An incision sits in or just above your existing crease, or where the surgeon plans to place a new one. A measured ellipse of skin is excised, sometimes with a sliver of underlying orbicularis muscle and a small amount of orbital fat. Your crease is then either preserved at its natural position or formed at a specifically designed new height. Recovery is fast, and the resulting scar hides within the fold when your eyes are open.
The effect on your eye is direct. Skin is shortened above the crease, your fold tightens, and your crease often becomes more defined. If you want a sharper, more visible double eyelid, this is the operation that produces it. If you want your existing eye shape preserved exactly, this is also the operation that may modify it.
If you have no crease at all and creating one is the actual goal, that is a different decision with its own logic, and our guide to incisional versus non-incisional double eyelid surgery walks through which eyelid belongs to which method.
Sub-brow lift (also called sub-brow blepharoplasty or infrabrow excision) removes a strip of skin from the sub-brow zone. An incision follows the inferior border of your eyebrow. A spindle-shaped ellipse of thick sub-brow skin is excised, the wound is closed, and your lid skin is effectively pulled upward toward the brow rather than the brow being pulled down onto your lid.
The effect on your eye is indirect. Your crease is not touched. Your lash position is unchanged. Your eye shape and eye opening look the same as before, only lighter and less hooded. What changes is the weight sitting above your fold. Long-term outcomes of subbrow blepharoplasty in Asian patients show it is especially effective for hooded upper eyelids, lateral hooding, descended brow tissue, and thick sub-brow skin.

Both procedures share recovery patterns. Stitches at five to seven days, mild bruising for one to two weeks, scar maturation over six to twelve months. Their difference is anatomical, not logistical.
Which One Is Right for You: Eight Patient Profiles
This section is the core of the decision. Most patients fall into one of the eight profiles below, or into a recognizable combination of two. Read them in order and identify which case most closely resembles your face.
Case 1: You Have a Monolid and Want to Stay a Monolid
You have a single eyelid with no visible crease, and you like your monolid eye shape. You have noticed that your upper lid feels heavier, hooded, and more tired than it used to. You want rejuvenation, but you do not want to be talked into a double eyelid operation. Your goal is to look fresher, not to become someone with different eyes.
Sub-brow lift is the right surgery for you. Because the incision sits at the inferior brow margin rather than across your lid, your monolid identity is preserved exactly. The heavy tissue weighing on your eye is removed from above, your lid feels lighter, and your face still looks like your face. Upper blepharoplasty would force the creation of a crease, which is not what you came for.
Case 2: You Have a Monolid and Want a Double Eyelid
You have a monolid, and you have decided that in addition to addressing the heaviness, you want a double eyelid created. That goal changes the calculus completely.
Upper blepharoplasty is the right operation for you, performed as a primary double eyelid procedure. Your surgeon designs both your new crease and the skin removal in a single operation, sometimes incorporating ptosis correction if your levator function warrants it. Sub-brow lift cannot create a crease and is not the operation for this goal.
Case 3: You Have a Natural Double Eyelid and Want Subtle Rejuvenation
You were born with a soft, natural-looking double eyelid. You like its subtle character. Now your lid feels heavier with age, your crease has softened slightly, and you want to look fresher without changing the impression your eyes give people. You specifically do not want a sharper, more pronounced crease.
Sub-brow lift is the right answer here. Upper blepharoplasty in this case would almost certainly deepen and sharpen your crease, producing a different eye impression than the one you have lived with all your life. Sub-brow lift addresses the heaviness from above without altering your natural crease architecture. Your eyes still read as your eyes, only lighter.
Case 4: Your Double Eyelid Has Faded and You Want It Sharper
You have always had a double eyelid, but over the years your crease has gotten shallow, low, or inconsistent. You miss the defined fold you remember from old photos. You want your crease back, sharper and more visible than it currently is.
Upper blepharoplasty is the operation you need. This is exactly the indication the procedure was designed for. Your surgeon removes redundant lid skin, reinforces the crease at the height you want, and produces a clear, defined double eyelid. Sub-brow lift would lift the weight off your fold but would not restore crease definition.
Case 5: You Had Double Eyelid Surgery Years Ago and Want to Preserve It
You had double eyelid surgery in your twenties or thirties. The result was beautiful, you have been happy with it for years, and now in your forties or fifties your lid has gotten heavier and your crease feels less defined. You do not want your previous surgery redone.
Sub-brow lift is the right approach for you. Re-entering the plane of an existing surgical crease disrupts the fixation that holds your fold in place, and the new healing rarely reproduces the same architecture. Revision blepharoplasty literature consistently identifies crease height change, asymmetry, triple folds, and the “sausage eye” pattern explained in our companion article on double eyelid revision and sausage eyes as common complications when this principle is ignored. Sub-brow lift never enters that plane. Your previous surgeon’s work stays exactly where it is, and the new heaviness is addressed from the brow side instead.
Case 6: Your Heaviness Is Concentrated in Lateral Hooding
Your inner lid looks reasonable, but the outer third of your eyelid carries a heavy fold of skin that sags over your outer canthus. Your eye looks smaller from the side, your eyeliner disappears under the hood, and the outer corner of your eye looks tired even when the rest of your face does not.
Sub-brow lift is the better choice for you, with the lateral portion of the excision extended outward to address the hooding directly. Upper blepharoplasty cannot reach the lateral fold effectively because the crease line does not extend far enough laterally to remove the descended sub-brow skin causing the hooding. Extended approaches that combine upper blepharoplasty with subbrow skin removal exist for severe cases, but for lateral hooding as the dominant finding, sub-brow lift alone is the more direct correction.
Case 7: Your Brow Itself Has Descended
You look in the mirror and your eyebrow position itself looks lower than it used to. Your brow tail sits closer to your eye. The heaviness you feel is brow weight pressing down rather than lid skin sagging up. Lifting your brow forcefully with your fingers dramatically opens up your eye.
Sub-brow lift is the procedure that fits your case, sometimes combined with a formal brow lift if descent is significant. Upper blepharoplasty in this scenario is the most common cause of an unsatisfying result, because it removes lid skin without addressing the source of the weight. Brow ptosis after upper blepharoplasty is so common, in fact, that recognizing brow descent preoperatively is one of the first things a board-certified plastic surgeon evaluates at consultation.
Case 8: You Have Heavy Tissue in Both Zones
You have thick descended sub-brow skin and clearly stretched, redundant lid skin. Neither operation alone fully addresses what you see in the mirror.
A combined procedure is the right approach for your situation, in which sub-brow lift addresses the upper component and a limited upper blepharoplasty (or a planned crease revision) addresses the lower component. Some surgeons stage these procedures across two operations; others perform them together depending on the severity. Asking a single procedure to do the work of two is one of the most common reasons severe dermatochalasis patients return dissatisfied.
Case 9: Your Upper Lid Looks Both Heavy and Hollow
You have a heavy upper eyelid, but at the same time the area just under your brow looks slightly sunken or hollow. The descended skin sits on top of a depleted sulcus. A standard sub-brow lift in this scenario can deepen the hollow it just removed skin from, leaving you with a result that feels emptier rather than refreshed.
Sub-brow lift is still appropriate for you, but it must be combined with volume preservation. Your surgeon may preserve or sculpt the underlying ROOF (the small fat pad beneath your orbicularis muscle) rather than removing it, or add a small fat graft to refill your sulcus. Combined approaches for dermatochalasis with sunken upper eyelids have become the standard of care in Korean plastic surgery for this presentation. The same principle applies to male patients, who generally want minimal brow elevation. Your surgeon designs the excision with reduced lateral extension and conservative skin removal, so the heaviness lifts without raising your brow into an unwanted feminized contour.
Surgeon’s Insight: The Principle of Dynamic Aesthetics
A common mistake patients make is choosing a procedure based on what they have heard about it rather than on what their face is actually doing. Sub-brow lift is not a trendier or more conservative version of upper blepharoplasty. Upper blepharoplasty is not a stronger or more thorough version of sub-brow lift. They are two structurally different operations addressing two structurally different patterns of aging.
Dynamic Aesthetics, the principle that your eyelid must look correct not only at rest but during every smile, every squint, every microexpression of conversation, demands that your surgeon read your anatomy first and choose the operation second. When the match is correct, your rejuvenation reads as a younger version of you. When the match is wrong, even a technically perfect operation produces an unsatisfying result, because the wrong tissue was addressed.
When Neither Surgery Is the Right Answer Yet
Two situations deserve specific caution before scheduling either procedure.
Subclinical ptosis. If underlying weakness in your levator muscle has been camouflaged by heavy skin for years, removing the skin reveals the ptosis instead of correcting it. Asian patients are particularly prone to this scenario, and surgery without preoperative levator evaluation often produces eyes that look smaller and sleepier after the operation. If your eyelid margin sits low against your pupil even when you raise your brow forcefully, ptosis repair belongs in your surgical plan alongside skin removal.
Significant brow descent. When your brow has dropped substantially, neither sub-brow lift alone nor upper blepharoplasty alone fully restores the youthful brow-lid relationship. A formal brow lift, endoscopic or open, may be the correct first procedure, with sub-brow lift or upper blepharoplasty added later if residual lid heaviness remains. Trying to compensate for significant brow descent through eyelid skin removal alone usually produces a temporary effect and a return to consultation within several years.
A careful examination by a board-certified plastic surgeon at consultation is the only reliable way to detect these conditions before they affect your result.
Specific Risks to Discuss at Consultation
No eyelid surgery is without risk, and an honest preoperative conversation covers the specific complications that have shaped how experienced surgeons design these procedures.
Eyebrow tail elevation. If your lateral sub-brow skin is removed too aggressively, the tail of your brow can lift unnaturally, producing a sharp or surprised expression that did not exist before. A conservative lateral design, individualized to your existing brow shape, prevents this outcome in most patients.
Sensory changes near the brow. Small sensory branches running through the sub-brow region can be stretched or interrupted during dissection. Temporary numbness of your brow area for several weeks is common. In a smaller number of patients, mild numbness persists for months. Permanent sensory loss is uncommon but possible.
Eyebrow hair loss. If the incision damages your hair follicles or the closure puts your brow under tension, you may develop a thinned strip along the lower brow margin. Proper beveled incision technique reduces this risk substantially.
A visible skin step-off. Because your brow skin is meaningfully thicker than your lid skin, the closure can show a small ridge or step-off for the first weeks to months. This usually softens with healing, but in patients with very thick skin a subtle step can persist.
Hypertrophic scar and pigmentation in darker skin. Asian skin (Fitzpatrick III to V) carries a higher risk of hypertrophic scarring and post-inflammatory hyperpigmentation than lighter skin. Your scar management protocol matters more than it would in lighter-skinned patients, and you should expect your surgeon to discuss it specifically.
Recovery and Realistic Expectations
Both procedures share similar recovery timelines, with small differences worth knowing.
Sub-brow lift (also called sub-brow blepharoplasty) is typically performed under local anesthesia with light sedation. Operating time runs about forty to sixty minutes for both eyes. Stitches come out at five to seven days. Bruising is usually mild and largely concealed by your brow itself. Most patients return to non-physical work within a week. Your scar line stays pink for three to six months and fades into the lower brow margin by the one-year mark in most patients with average healing.
Upper blepharoplasty follows nearly the same timeline. Stitches at five to seven days, work return at one week for office-based jobs, residual swelling for two to four weeks. Your scar sits in the crease and hides within the fold when your eyes are open, though it can be visible when you look downward for the first six to twelve months.
Long-term durability is good for both procedures when the operation is matched to the correct zone, because the descended tissue has been physically removed rather than simply tightened. Most patients see their result well-maintained for many years, though continued aging means small change over time is normal in both.
Scar care matters more in Asian skin than in lighter skin, where hypertrophic scarring and pigmentation are more common. Most surgeons recommend silicone gel or silicone sheets for the first two to three months and strict sunscreen for at least six months. If your scar starts to thicken or darken at any point, early steroid injection can keep it from progressing further. Avoiding heat, friction, and direct sun exposure on the healing scar for the first eight weeks is the single most useful thing you can do at home.
Match the Operation to the Source, Not to the Symptom
This decision is not about which procedure is more popular, more advanced, or more aggressive. This decision is about which procedure matches the anatomy and the goal you actually have. Sub-brow lift and upper blepharoplasty are not competitors. They are complementary tools, each correct for a specific subset of patients and incorrect for the rest.
If you recognized yourself clearly in one of the eight patient profiles above, you now have a working hypothesis to bring to consultation. If you recognized yourself in more than one or in none, an in-person examination by a board-certified plastic surgeon will resolve the ambiguity, with assessment of your brow position, your sub-brow skin thickness, your lid skin redundancy, your levator function, and any prior surgical crease.
For related decisions in eyelid surgery, our guide to double eyelid revision and sausage eyes extends the same anatomy-first principle to crease-level revision, and our comparison of lower blepharoplasty versus tear trough fillers applies it to the lower eyelid. In Korean plastic surgery practice, preoperative marking is performed with you sitting upright and awake, so your true brow position and your natural dynamic expression guide the design of each incision. The principle is constant: match the operation to the source, not to the symptom.
Written by Dr. Yongwoo Lee, board-certified Korean plastic surgery specialist in facial anatomy and aesthetic procedures at VIP Plastic Surgery, South Korea.
Frequently Asked Questions About Sub-Brow Lift vs. Upper Blepharoplasty
I have a monolid and don’t want a double eyelid. Can sub-brow lift help me look less tired?
Yes, and this is one of the strongest indications for the procedure. Sub-brow lift removes a strip of thick skin from beneath your eyebrow without ever touching your lid, your lash line, or the area where a crease would be formed. Your monolid identity is preserved exactly, while the weight pressing down on your upper eyelid is reduced. Patients who specifically do not want a double eyelid created, but who are tired of looking heavy or older around the eyes, are often the ideal candidates for sub-brow lift. Upper blepharoplasty would necessarily create or define a crease and is not the right operation for this goal.
My double eyelid has gotten shallow with age. Should I get a sub-brow lift or a revision upper blepharoplasty?
That answer depends on how the change happened. If your crease has lost definition because heavy sub-brow tissue has descended over the top of it, sub-brow lift addresses the cause directly without disturbing your original fold. If your crease has lost definition because the fixation itself has loosened or the height has dropped, a revision upper blepharoplasty may be needed to reinforce the architecture. In Korean plastic surgery practice, the conservative approach is to attempt sub-brow lift first when descended sub-brow tissue is the dominant finding, because re-entering the original crease plane carries its own risks. A board-certified plastic surgeon will distinguish between these two patterns at consultation.
Will sub-brow lift change the shape or size of my eyes?
No. Your incision sits at the inferior edge of your eyebrow, well above your lid, and it never crosses or modifies the structures that define your eye shape. Your lash line, your crease, your lateral canthus, and the curvature of your palpebral opening are all preserved exactly. What changes is the weight sitting above your fold, which produces a visual effect of lighter, more open eyes without altering the geometry that makes your eyes recognizable as yours. Patients who specifically want rejuvenation without any change in eye shape choose sub-brow lift for this reason.
Can I get sub-brow lift after I’ve already had double eyelid surgery?
Yes, and this is one of the most common scenarios in Korean plastic surgery practice. Patients who had double eyelid surgery in their twenties and now want rejuvenation in their forties or fifties are often better served by sub-brow lift than by another operation through the crease, because re-entering the original surgical plane risks crease height change, asymmetry, triple folds, or the “sausage eye” pattern. Sub-brow lift addresses the new heaviness from above while leaving your original crease completely untouched. For most patients with a satisfactory prior result, sub-brow lift is the safer rejuvenation pathway.
Which procedure has the shorter recovery and the less visible scar?
Recovery timelines are nearly identical. Both procedures involve stitches at five to seven days, mild bruising for one to two weeks, and scar maturation over six to twelve months. Scars are also both inconspicuous in most patients when properly designed, though they sit in different locations. Sub-brow lift leaves a scar at the inferior brow margin, concealed by the natural shadow of the brow and by eyebrow hair growing across it. Upper blepharoplasty leaves a scar within the crease, concealed by the fold when your eyes are open. Neither has a meaningful advantage in recovery speed.
How do I know if I have brow ptosis instead of just heavy lids?
A simple test is to relax your forehead completely, then use a fingertip to lift your brow gently to its natural arched position while looking in the mirror. If raising the brow produces a dramatic improvement in your upper eyelid heaviness, your heaviness is largely driven by brow descent rather than by isolated lid skin excess. If the same lift produces only modest change, your heaviness sits more in the lid zone itself. Relaxing the forehead matters, because forcefully raising your eyebrows recruits the frontalis muscle and lifts the skin in a way that can blur the distinction. A board-certified plastic surgeon performs this evaluation systematically at consultation, measuring your brow height relative to the supraorbital rim and assessing how much weight transfers between zones. Many patients have a mix of both, in which case the proportion guides the surgical plan.
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified medical professional before making any decisions about surgical or non-surgical procedures.