The One Word Every Facelift Surgeon Watches For
Of every complication that can follow facial rejuvenation surgery, hematoma is the one your surgeon thinks about most. It is not the most common outcome, but it is the one that determines whether your recovery is uneventful or unexpectedly difficult. If you are researching facelift surgery and trying to understand the real risks, this is the conversation that deserves your full attention. The most honest sentence any plastic surgeon can say to you is this: “Hematoma after facelift is the complication we work hardest to prevent, because we know exactly what causes it.”
A facelift hematoma is a collection of blood that accumulates beneath your skin in the space the surgeon dissected during the operation. According to the American Society of Plastic Surgeons, facelift surgery remains one of the most established and refined procedures in modern aesthetic medicine, and reported hematoma rates have steadily declined as surgical technique has matured. Even so, no operation that elevates large soft tissue flaps over a vascular surface can ever be entirely risk-free. What separates a safe, predictable result from a difficult recovery is whether your surgeon has built every step of the procedure around hematoma prevention. A 2023 review titled “Hematomas and the Facelift Surgeon” frames this as the central safety responsibility of any rhytidectomy practice.
This article walks you through what a facelift hematoma actually is, how it differs from a seroma, why your face is particularly vulnerable to it, the role uncontrolled blood pressure and other risk factors play in nearly every serious case, the layered prevention strategy a board-certified plastic surgeon uses inside and outside the operating room, the modern mapping suture technique that has further reduced the risk in recent years, the role of closed-suction drains in combined facelift and neck lift cases, and the treatment pathway if a collection does develop.
What a Facelift Hematoma Actually Is
During a facelift, your surgeon elevates the skin and the underlying SMAS (Superficial Musculoaponeurotic System) layer off the deeper structures of your face. This dissection creates a temporary potential space between the lifted tissue and the structures below it. Under normal healing, that space closes within hours as the tissues lay back down and small vessels seal.
A hematoma forms when a vessel that was sealed during surgery reopens after the operation, or when a small uncontrolled vessel continues to ooze after closure. Blood accumulates in the dissected space and produces swelling, pressure, asymmetry, and pain that is disproportionate to your normal postoperative discomfort. In its most concerning form, called an expanding hematoma, blood accumulates rapidly and visibly distorts one side of your face within hours of surgery. This represents a true surgical emergency and requires immediate return to the operating room for evacuation and control of the bleeding source.
A close cousin of hematoma is seroma, in which clear, straw-colored serous fluid rather than blood collects in the same dissected space. Seromas tend to be less painful and less urgent than hematomas, but they share the same underlying problem of an unobliterated dead space. Reassuringly, the modern prevention strategies you will read about below, including the mapping suture and closed-suction drains, address both conditions simultaneously.
Most clinical literature places the overall hematoma rate after facelift somewhere between one and eight percent, depending on the technique used, the patient population, and the rigor of perioperative blood pressure management. Within that statistic, expanding hematomas requiring emergent reoperation are far less common than smaller, late-presenting collections. Both ends of the spectrum, however, demand a deliberate management plan.
Why Hematoma Is the Complication Surgeons Take Most Seriously
A hematoma is not simply a bruise that will fade with time. When blood pools beneath the lifted facial flap, several distinct problems can unfold if the collection is not recognized and treated correctly. A comprehensive review of “How to Prevent and Treat Complications in Facelift Surgery” details each of these consequences and their long-term aesthetic impact.
Pressure on the overlying skin is the most immediate concern. Your facial skin after a facelift survives on a delicate blood supply that has been partially interrupted by the dissection. When a hematoma generates internal pressure against that thin, healing flap, it can compromise the circulation enough to cause skin flap necrosis, a localized loss of tissue that produces visible scarring and pigmentation changes long after the original surgery has healed. This is the outcome every facelift surgeon is determined to prevent.
A persistent hematoma can also distort the way your tissue heals. Blood breakdown products are inflammatory, and when they sit in contact with the dissected planes for days, they can trigger a fibrotic response that leaves you with firmness, irregular contour, or an uneven jawline weeks after the bruising itself has resolved. In some cases, residual blood that does not absorb fully organizes into a fibrous mass that requires surgical revision to correct.
Less commonly, a hematoma can become a nidus for infection, since blood is an ideal medium for bacterial growth. And in cases where the collection extends near the auricular region, it can contribute to the very deformities, including pixie ear and irregular incision lines, that careful facelift planning is supposed to avoid. You can read more about how those secondary deformities develop in our discussion of facelift side effects and the windblown look.
The Anatomy of Bleeding: Why Your Face Is Particularly Vulnerable
To understand why hematoma prevention requires such layered planning, it helps to appreciate how vascular your face actually is. The facial soft tissues receive blood through a dense network of branches from the external carotid artery, including the superficial temporal, facial, and posterior auricular arteries, all of which branch and anastomose extensively across the field your surgeon is working in. This rich blood supply is what allows your facial skin to heal quickly and reliably after surgery, but it also means that any vessel left unsealed has the potential to bleed.
Two anatomical realities make facelift dissection unique. First, the dissection plane crosses many small perforating vessels that connect the deep tissues to the skin flap above. Each one must be cauterized or ligated. Second, once the flap is elevated, a real dead space exists between the underside of your skin and the SMAS or deeper tissue beneath it. Even if every vessel is sealed at the moment of closure, that dead space is a reservoir waiting to fill if a vessel reopens later.
Two postoperative events most commonly cause sealed vessels to reopen: a sudden surge in your blood pressure, and any forceful Valsalva maneuver, meaning coughing, vomiting, retching, straining, or shouting. Both events can momentarily exceed the holding force of the cautery seal on a small vessel, allowing blood to escape into the surgical pocket. This is why the hours immediately following your facelift are managed with such deliberate quietness, head elevation, antiemetics, and tightly controlled blood pressure.
Hypertension and the Other Risk Factors That Multiply Your Hematoma Rate
Decades of facelift outcome data have identified a small group of patient and behavioral factors that meaningfully increase your individual risk. A board-certified plastic surgeon screens for every one of these during your preoperative evaluation. Comprehensive evidence-based reviews, including the “Methods for Minimizing Bleeding in Facelift Surgery” review, converge on the same hierarchy of risk.
Uncontrolled Hypertension: The Dominant Risk
Among every variable that influences your hematoma risk, uncontrolled blood pressure stands above all others. Patients whose blood pressure is poorly managed before, during, and after surgery experience hematoma at substantially higher rates than patients whose blood pressure is well controlled. A single-surgeon series of 118 consecutive facelifts found that intraoperative systolic blood pressure was an independent predictor of postoperative hematoma, reinforcing what the broader literature has demonstrated for decades.
Mechanically, the picture is straightforward. Higher arterial pressure exerts more force on the surgically sealed vessels along your dissection plane. A vessel that would hold reliably at a systolic pressure of 120 mmHg may rupture at a systolic pressure of 180 mmHg. Even transient surges, the kind that occur during emergence from anesthesia, during straining, or in response to anxiety and pain, can be sufficient to dislodge a clot and initiate bleeding into your facial flap.
For this reason, a board-certified plastic surgeon will require a thorough cardiovascular evaluation before scheduling your facelift if you have any history of hypertension. Your blood pressure must be optimized on a stable, well-tolerated regimen before surgery is approved. If your pressure is not adequately controlled at the time of your preoperative visit, your surgery will be delayed, not rushed. This delay reflects a calculated decision based on the same risk data your surgeon uses every day to keep your recovery uneventful. A surgery delayed by two weeks while your medication is adjusted is far preferable to a hematoma that complicates your healing for months.
Male Sex
Men experience hematoma after facelift at meaningfully higher rates than women, with multiple large series reporting incidences two to several times higher in male patients. Anatomical factors explain this. Male facial skin tends to be thicker and more vascular, particularly across the beard distribution where dense follicular blood supply runs through the dissection plane. Male patients also tend to carry higher baseline blood pressures and more variable cardiovascular profiles. None of this disqualifies men from facelift surgery, and modern outcomes in male patients are excellent. What it does mean is that a serious surgeon applies tighter perioperative protocols, more aggressive intraoperative hemostasis, and more vigilant early postoperative monitoring when the patient is male.
Smoking, Sleep Apnea, and Hormonal Factors
Several additional conditions tilt your risk profile and deserve direct attention before surgery is scheduled.
Smoking and nicotine exposure affect facelift safety on multiple fronts. Nicotine causes vasoconstriction that compromises the perfusion of the elevated skin flap, increases the risk of skin necrosis, and prolongs healing. Smokers also tend to cough more frequently in the postoperative window, and each forceful cough is a Valsalva event that stresses the hemostatic seals along your dissection. A responsible surgical practice requires complete cessation of cigarettes, vaping, nicotine patches, and nicotine gum for at least four to six weeks before surgery and for at least two weeks afterward. This is not a preference. It is a non-negotiable safety prerequisite.
Obstructive sleep apnea (OSA) raises hematoma risk in a way many patients do not anticipate. During apneic episodes, blood pressure can spike substantially, and these surges occur most often at night during the very window in which sealed vessels are most vulnerable. If you have diagnosed sleep apnea, your CPAP device should be brought to your recovery and used as prescribed during the first nights of healing. If you have suspected but undiagnosed OSA, a sleep evaluation before surgery is reasonable.
Hormone replacement therapy and estrogen-containing contraceptives have been associated with elevated bleeding risk in some studies, and many practices recommend pausing them for two to four weeks before surgery in coordination with your prescribing physician.
A general principle ties these factors together. The closer your physiology is to a calm, well-controlled baseline at the moment your surgeon begins the operation, the lower your hematoma risk will be at every stage of recovery.
Surgeon’s Insight: The Principle of Redundant Safety
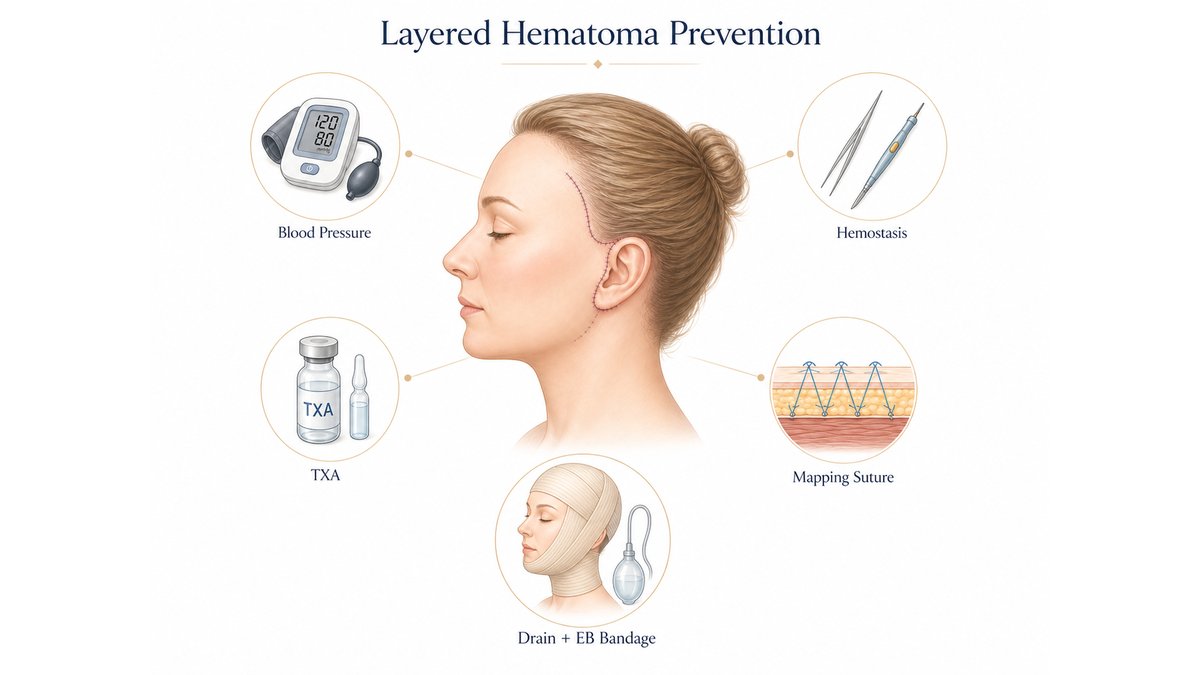
Among aesthetic surgeons, there is a quiet understanding that no single intervention is sufficient to eliminate hematoma. What works is layered redundancy: blood pressure optimization, careful medication review, meticulous intraoperative cautery, intravenous and topical hemostatic agents, the mapping suture, closed-suction drains, the compression dressing, and the activity discipline of the first twenty-four hours. Each layer addresses a different mechanism of bleeding, and each layer is engineered to absorb the failure of any other layer. This is the principle of Redundant Safety, and it is the unspoken architecture of every facelift practice that consistently delivers safe, beautiful results.
What this means for you, as the patient, is that the surgeons who achieve the most reliable outcomes are not necessarily the ones whose techniques look most innovative on social media. They are the ones who have built every layer of this system into their daily protocol and refuse to skip any of them. When you evaluate a surgeon, you are not just evaluating their hands. You are evaluating whether they have engineered a perioperative protocol that protects you even on the rare day when a single vessel behaves unexpectedly.
Prevention Begins Long Before You Enter the Operating Room
The work of preventing a facelift hematoma starts at your first preoperative visit, weeks before the day of surgery. A careful surgeon will review every medication and supplement you take and identify any that increase bleeding risk, which is a longer list than most patients realize. Aspirin, ibuprofen, naproxen, and other nonsteroidal anti-inflammatory medications all impair platelet function. Many over-the-counter supplements, including fish oil, vitamin E in high doses, ginkgo biloba, garlic extract, ginseng, and turmeric, exert similar effects. Anticoagulant prescriptions such as warfarin, apixaban, and rivaroxaban require coordinated management with your prescribing physician.
You will be asked to discontinue these substances on a defined timeline before your facelift, typically two weeks for aspirin and supplements, with longer washout periods for prescription anticoagulants depending on the specific drug. This step ranks among the highest-yield interventions in your prevention plan.
Alongside medication review, your surgeon will assess your baseline blood pressure, your cardiovascular history, your tobacco and alcohol use, and any condition that might affect coagulation, including the risk factors discussed above. If anything in this evaluation suggests elevated risk, additional optimization steps will be added to your plan before the date of surgery is confirmed.
Inside the Operating Room: How Surgeons Stop Bleeding Before It Starts
Once you are asleep, the prevention strategy continues with a level of meticulousness that defines the difference between a careful facelift and a rushed one. Several layered interventions are at work simultaneously.
Meticulous Hemostasis at Every Step
The single most important intraoperative variable is how thoroughly your surgeon controls bleeding as the dissection proceeds. Every small perforating vessel that crosses the dissection plane is identified and sealed, either with bipolar electrocautery or with fine ligation. A surgeon who is willing to slow down at this stage, methodically working across the entire flap before proceeding to closure, builds the foundation of a hematoma-free recovery. This step cannot be hurried without consequence.
Topical Hemostatic Agents
Beyond cautery, modern facelift surgery makes routine use of topical hemostatic agents applied directly to the surgical field. These products, including oxidized cellulose, gelatin matrices, and fibrin sealants, accelerate clot formation at the level of the smallest vessels that are too fine to ligate. They are particularly valuable along the broad surface of the dissected flap, where diffuse oozing can otherwise contribute to a slowly developing collection.
Intravenous Hemostatic Agents: Tranexamic Acid and Botropase
Two intravenous medications work alongside meticulous cautery and topical hemostatics to form the modern multimodal approach to bleeding control.
Tranexamic acid (TXA) has become a cornerstone of bleeding control in modern plastic surgery. By inhibiting the breakdown of clots that have already formed, TXA stabilizes the hemostatic seals at every cauterized vessel along your dissection. Multiple peer-reviewed studies have demonstrated meaningful reductions in intraoperative blood loss, postoperative bruising, and hematoma rates when TXA is administered during facelift surgery. A scoping review of tranexamic acid in rhytidectomy and a broader systematic review of TXA in aesthetic facial plastic surgery both confirm a favorable safety profile alongside reduced bleeding outcomes. TXA is now considered a standard adjunct in many high-volume aesthetic practices and is delivered intravenously, topically, or in tumescent solution depending on the surgeon’s protocol.
Botropase, a hemocoagulase derived from snake venom, is widely used in Korean plastic surgery and across much of Asia as an additional intraoperative hemostatic agent. Administered intravenously, it activates clot formation at the local injury site without producing systemic hypercoagulability. Used alongside TXA and meticulous cautery, Botropase contributes to a measurable reduction in capillary oozing across the dissected facial flap, which translates directly into a lower hematoma risk during the early postoperative window.
The combination of these two agents reflects a deliberate philosophy: TXA stabilizes existing clots, Botropase encourages new clot formation at active bleeding sites, and the two together address the bleeding problem from both ends of the coagulation pathway.
Smooth Anesthetic Emergence
The transition from general anesthesia back to wakefulness is one of the highest-risk windows for a hematoma to begin. Coughing, bucking on the endotracheal tube, retching, and sudden blood pressure surges during emergence can dislodge sealed vessels at the very moment your wound has just been closed. A modern anesthesia team plans for this from the moment your case begins. They use careful agent selection to allow a smooth wake-up, prophylactic antiemetics to prevent vomiting, deep extubation techniques where appropriate, and tight blood pressure control through emergence and into the recovery room. The result is a quiet, smooth transition that protects the work the surgeon has just completed.
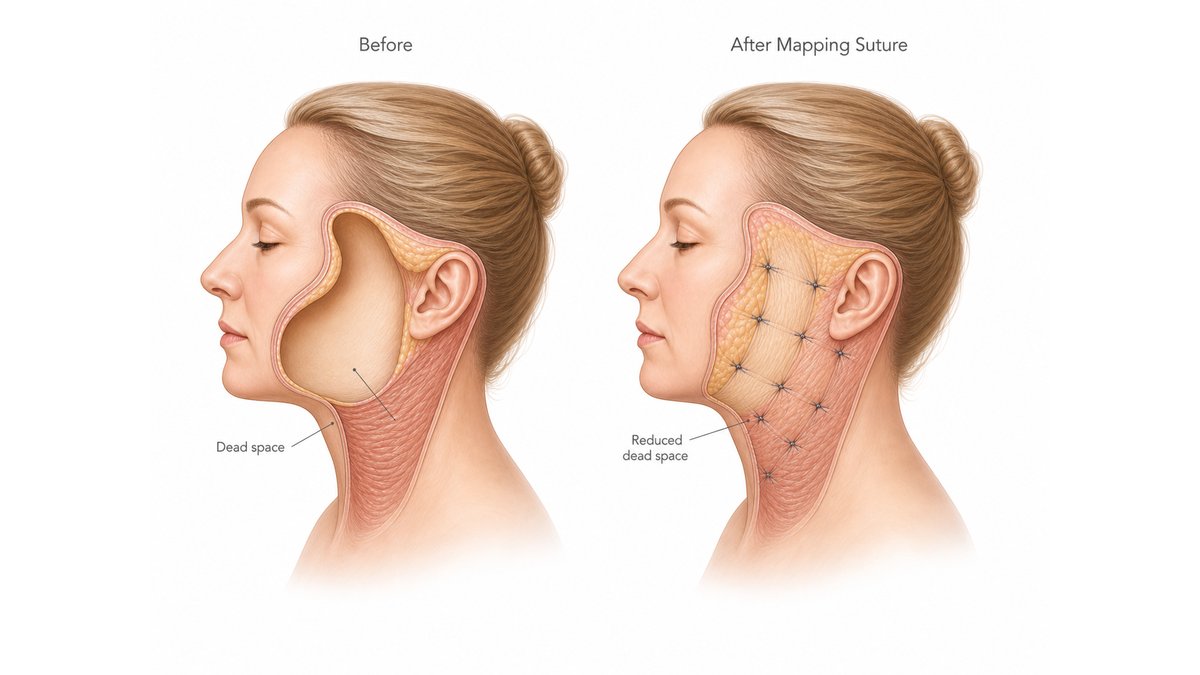
The Mapping Suture: Closing the Dead Space Mechanically
One of the most significant recent refinements in facelift safety is a closure technique known by several interchangeable names in the literature: mapping suture, quilting suture, progressive tension suture (PTS), external quilting suture, and the hemostatic net (the variant first popularized by the Brazilian surgeon Auersvald, sometimes called the Auersvald net). The principle is shared across these terms, and the impact on hematoma and seroma prevention has been substantial. A systematic review of quilting sutures in rhytidectomy and the original report on external quilting sutures preventing hematomas in cervicofacial rhytidectomies both document meaningful reductions in hematoma rate when the technique is applied.
After the facelift dissection is complete and hemostasis has been achieved, your surgeon places a series of fine 4-0 nylon sutures that pass from the underside of the skin flap down to the SMAS or other firm base tissue beneath. In the hemostatic net variant, the same nylon sutures are placed from the outside of the skin in a grid pattern, again anchoring the skin to deeper tissue at multiple points. Either approach distributes the sutures across the entire dissected territory and tacks the elevated skin to the underlying scaffolding before the final skin closure is completed.

Anatomically, this works elegantly. Remember that a hematoma requires a dead space to fill. By tacking the skin flap directly down to the SMAS at numerous discrete points, the mapping suture closes the dead space mechanically. There is simply no longer a meaningful pocket for blood or serous fluid to accumulate in. Even if a small vessel were to ooze in the postoperative period, the volume it could deposit before encountering tissue contact is minimized. This same mechanism protects you against seroma formation in parallel.
This technique offers a second benefit beyond hematoma and seroma prevention: it distributes the tension of the lift across the entire flap rather than concentrating it along the incision line. This more even tension distribution contributes to a more natural-looking result and reduces the risk of widened or hypertrophic scars. You can read more about how incision design influences scar quality in our article on deep plane facelift scars and incision healing.
The mapping suture does not replace the other layers of prevention. It works alongside meticulous cautery, hemostatic agents, tranexamic acid, blood pressure control, drains, and compression dressing. What it adds is a mechanical safeguard that addresses the anatomical vulnerability at its root, the dead space itself.
Closed-Suction Drains: Active Evacuation in the Early Recovery Window
Closed-suction drains complement the mapping suture by addressing a different aspect of the same problem. Where the mapping suture mechanically obliterates the dead space, the drain actively evacuates whatever residual fluid still emerges from sealed vessels and capillary networks during the first day of healing.
The number of drains placed depends on the scope of your procedure. In a deep plane facelift combined with a neck lift, a careful surgeon typically places two closed-suction drains per side, with one positioned in the lateral cheek and SMAS region and the other in the postauricular and cervical territory. When the procedure is limited to the face without a separate neck dissection, a single drain per side is generally sufficient. The drains themselves are small, soft, bulb-suction devices, often referred to as Jackson-Pratt or comparable systems, brought out through small stab incisions placed inconspicuously behind the ear.
Mechanically, the principle is intuitive. Each drain creates a low, continuous negative pressure across the dissected pocket, drawing any blood or serous fluid away from the tissue planes before it can accumulate. The drains are typically removed within 24 to 48 hours, once the output has tapered to a clinically insignificant volume. Their presence over the first night is one of the most reliable indicators that any oozing is being captured rather than collecting silently.
A reasonable question patients sometimes ask is whether the mapping suture and drains are redundant. The honest answer is that they are complementary, not redundant. The mapping suture closes the space; the drain captures any fluid that still emerges before the tissues have fully bonded. In high-risk patients, in larger combined procedures, and in cases where the surgeon prefers maximum safety margin, both are routinely used together.
The Compression Dressing and the Activity Discipline of the First Twenty-Four Hours
After your incisions are closed and any drains are secured, your face is wrapped in a carefully applied compression dressing that remains in place through the first night and the morning that follows. This dressing is not a cosmetic afterthought. This dressing functions as a deliberate hemostatic tool.
By applying gentle, even pressure across the entire dissected territory, the compression dressing reinforces the same principle the mapping suture addresses internally: it minimizes the space available for blood to accumulate. It also dampens the small pressure fluctuations that occur with normal head movement, providing an additional margin of stability during the critical hours when sealed vessels are most likely to reopen.
Beyond the dressing itself, the first night carries specific behavioral instructions, and following them precisely is one of the most important contributions you make to your own outcome. You will sleep with your head elevated on multiple pillows or in a recliner at thirty to forty-five degrees, a position that reduces venous pressure across the surgical field. Bending forward, lifting anything heavier than a few pounds, and sudden head movements are restricted for several days. Exercise, particularly anything that elevates your heart rate or blood pressure, is restricted for one to two weeks. Sexual activity is restricted for the same window. Hot showers, saunas, alcohol, and any activity that could raise blood pressure or trigger nausea are avoided.
Your team will also provide pain control and antiemetic medications calibrated to keep you comfortable, because pain itself raises blood pressure, and nausea risks a Valsalva event. Specific symptoms that should prompt an immediate call include disproportionate pain on one side, rapidly increasing swelling, a sense of tightness, or any visible difference between the two sides of your face. Early recognition of those signs is the single most important factor in protecting your final result from a developing hematoma.
What Happens If a Hematoma Develops Anyway
Even with every prevention measure in place, no surgical protocol can promise a zero hematoma rate. What a comprehensive protocol does promise is rapid recognition and decisive treatment if a collection develops, which is what determines whether your final result is affected.
A small, late-presenting hematoma that does not expand and does not threaten your skin flap can often be managed conservatively. Your surgeon may aspirate the collection with a fine needle in the office, sometimes followed by an injection of medication to help your body absorb the residual blood. Serial visits over the following one to two weeks ensure that the collection resolves fully and that no organized clot remains.
A larger collection, or one that does not absorb after aspiration, may require revision surgery to evacuate the residual hematoma, irrigate the pocket, and confirm that no active bleeding source remains. This is a relatively brief procedure compared with the original facelift, and when performed promptly, it allows your final aesthetic outcome to remain intact.
An expanding hematoma, where blood is accumulating rapidly and visibly distorting one side of your face within hours of surgery, is treated as a true surgical emergency. You will be returned immediately to the operating room, the incisions reopened, the accumulated blood evacuated, the responsible vessel identified and controlled, and the flap reclosed. With prompt management, even an expanding hematoma rarely affects the long-term aesthetic result. The danger is in delay, not in the hematoma itself.
This is why your surgical team will give you specific symptoms to watch for and why the first twenty-four hours are managed with such close monitoring. A hematoma that is recognized early and treated promptly leaves no permanent footprint. A hematoma that is recognized late is what causes the problems your surgeon is trying so hard to prevent.
Hemostasis Is the Quiet Foundation of a Beautiful Result
A successful facelift is often discussed in terms of vector, plane, ligament release, and contour. All of these matter. But the prerequisite for any of them to translate into a durable, natural-looking outcome is uneventful healing, and uneventful healing depends on the absence of hematoma.
Everything you have read here, the preoperative medication review, the blood pressure optimization, the careful screening for male sex, smoking, sleep apnea, and hormonal factors, the meticulous intraoperative hemostasis, the tranexamic acid and Botropase, the smooth anesthetic emergence, the mapping suture or hemostatic net, the closed-suction drains, the compression dressing, and the activity discipline of the first twenty-four hours, exists for one purpose. Each layer exists so that the artistry your surgeon performs at the level of the SMAS, the retaining ligaments, and the skin flap can heal exactly as it was designed to.
If you are evaluating facelift surgeons, the questions that distinguish a careful practice from a rushed one are not the ones about technique alone. They are the ones about protocol. How is your blood pressure managed in the days before and after surgery? What hemostatic agents are used during the case? Is the mapping suture or hemostatic net part of the closure? How many drains are placed for your specific procedure? What is the team’s plan if a hematoma is suspected? In Korean plastic surgery, where anatomical precision and rigorous perioperative protocols define the standard of care, these are the questions a serious surgeon will answer in detail. For a deeper look at how surgical philosophy shapes the visible result, our comparison of Deep Plane and SMAS facelift techniques is a useful next step.
Written by Dr. Yongwoo Lee, board-certified Korean plastic surgery specialist in facial rejuvenation and aesthetic surgery at VIP Plastic Surgery, South Korea.
Frequently Asked Questions About Facelift Hematoma
What does a facelift hematoma feel like?
A facelift hematoma usually presents as disproportionate, asymmetric swelling on one side of your face, often accompanied by pain that feels significantly worse than your normal postoperative discomfort. You may notice a sense of tightness, fullness, or pressure that develops over a short window of time, sometimes within hours of surgery. The affected side may look firm or feel different to the touch compared with the unaffected side. Any of these signs in the first day or two after your facelift should prompt an immediate call to your surgical team. Early recognition is the single most important factor in preventing a hematoma from affecting your long-term aesthetic result.
How common is hematoma after a facelift?
Reported hematoma rates after facelift surgery generally fall between one and eight percent, depending on the surgical technique, the patient population, and how rigorously perioperative blood pressure is managed. Within that range, expanding hematomas requiring emergency reoperation are substantially less common than smaller, late-presenting collections that can be managed conservatively. Modern advances, including intravenous tranexamic acid, the mapping suture or hemostatic net technique, the routine use of closed-suction drains in combined procedures, and tighter blood pressure protocols, have meaningfully lowered hematoma rates in high-volume aesthetic practices over the past decade.
When does a facelift hematoma usually occur?
The vast majority of clinically significant facelift hematomas develop within the first twenty-four hours after surgery, and most within the first six to twelve hours. This is the window in which sealed vessels are most vulnerable to reopening, particularly in response to a blood pressure surge or a Valsalva maneuver such as coughing, vomiting, or straining. A smaller proportion of hematomas present later, sometimes several days into recovery, and these are typically slower-developing collections from low-pressure vessels or persistent capillary oozing. Your surgical team monitors you most intensively during the first day after surgery, and the postoperative instructions you receive emphasize quiet, restricted activity during that window.
Are men at higher risk of hematoma after facelift surgery?
Yes. Multiple large series have demonstrated that male patients experience hematoma after facelift at meaningfully higher rates than female patients, with some reports showing a several-fold increase in incidence. Anatomy explains this gap. Male facial skin tends to be thicker and more vascular, particularly across the beard distribution where dense follicular blood supply runs through the dissection plane. Men also tend to carry higher baseline blood pressures and more variable cardiovascular profiles. None of this disqualifies men from facelift surgery, and modern outcomes in male patients are excellent. What it does mean is that a careful surgeon applies tighter perioperative blood pressure control, more aggressive intraoperative hemostasis, and more vigilant early postoperative monitoring when the patient is male.
Can high blood pressure cause hematoma after a facelift?
Yes. Uncontrolled hypertension is the single most important modifiable risk factor for facelift hematoma. Higher arterial pressure increases the mechanical force on every vessel that was sealed during your surgery, and even transient pressure surges during emergence from anesthesia, in response to pain, or during straining can be sufficient to dislodge a clot and initiate bleeding into the surgical pocket. For this reason, a board-certified plastic surgeon will require your blood pressure to be optimized on a stable regimen before scheduling your facelift, and will delay surgery if your pressure is not adequately controlled at the time of your preoperative visit. This delay is not excessive caution. It is one of the highest-yield safety decisions in your entire surgical plan.
What is a mapping suture in facelift surgery?
A mapping suture, also called a quilting suture, progressive tension suture, external quilting suture, or hemostatic net (the Auersvald net being a well-known variant), is a closure technique that uses fine 4-0 nylon sutures to anchor the underside of the lifted skin flap directly to the SMAS or other firm base tissue beneath it, at multiple discrete points across the dissected territory. Because a hematoma requires a dead space to accumulate in, the mapping suture mechanically closes that dead space and dramatically reduces the volume that any postoperative bleeding could occupy. The same mechanism also reduces seroma formation. This technique distributes the tension of the lift more evenly across the entire flap, which contributes to a more natural-looking contour and helps minimize the risk of widened or hypertrophic scars at the incision lines.
Are drains always used after a facelift?
Drain use depends on the scope of your procedure and your surgeon’s protocol. In a deep plane facelift combined with a neck lift, two closed-suction drains per side are commonly placed, one in the lateral cheek and SMAS region and one in the postauricular and cervical territory, to actively evacuate any residual blood or serous fluid from the larger dissected territory. When the procedure is limited to the face without a separate neck dissection, a single drain per side is generally sufficient. The drains are small, soft, bulb-suction devices brought out through inconspicuous stab incisions behind the ear, and they are typically removed within 24 to 48 hours once the output has tapered. Drains are complementary to the mapping suture, not redundant with it. The suture closes the dead space mechanically, while the drain captures any fluid that still emerges before the tissues have fully bonded.
Can a facelift hematoma be prevented completely?
No surgical protocol can guarantee a zero hematoma rate, and any surgeon who promises one is not being fully honest with you. What a rigorous, modern protocol does deliver is a hematoma rate that has been driven as low as the current state of the art allows, layered with rapid recognition and decisive treatment if a collection does develop. The combination of preoperative blood pressure optimization, careful medication review, screening for male sex and other risk factors, intraoperative tranexamic acid and Botropase, meticulous hemostasis, smooth anesthetic emergence,
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified medical professional before making any decisions about surgical or non-surgical procedures.