The One Question Every Fat Transfer Patient Asks
Fat grafting sells itself on a beautiful idea: take fat from where you do not want it and move it to where you do, using your own living tissue instead of an implant or a filler. What almost no consultation explains clearly is the fine print. Not all of the fat you pay to have transferred actually stays. Some of it never gets a blood supply, dies quietly in the first weeks, and is reabsorbed by your body. The number that matters for your result is not how many cubic centimeters go in on the day of surgery. What counts is how much is still alive months later.
The short answer: plan on roughly half of the transferred fat surviving long term, with published ranges from about a third to two thirds depending on the area and the technique. Whatever lasts past six months is permanent. The rest is reabsorbed in the first few months, which is exactly why experienced surgeons deliberately overfill.
That gap between what is injected and what survives is the single biggest source of disappointment in fat transfer, and also the single most avoidable one. When you understand fat graft survival before your procedure, you stop expecting the day-one volume to be your final result, you read the early deflation as normal rather than as failure, and you can tell a realistic plan from an overpromise.
This guide walks you through the honest numbers. You will learn how a fat graft actually takes, roughly how much survives in the breast, the buttock, and the face, when the loss happens, what makes the difference between a graft that lasts and one that melts away, and what you can do to protect your result.
The Real Number Is Retention, Not Injection
Most patients think about fat transfer in terms of the amount injected. A better frame is retention: the percentage of that fat still present and alive after your body has finished its natural resorption. A surgeon who injects 300cc into each breast and keeps half has delivered the same lasting result as one who injects 200cc and keeps three quarters. Injected volume is a starting bid. Retention is the settlement.
This reframing changes how you read a plan. If two surgeons quote very different injection volumes, the larger number is not automatically the better result, because it may simply reflect a plan that expects heavier loss. The questions worth asking are about technique, staging, and realistic expected retention for your area, not about who promises to inject the most on the day.
Do You Have Enough Fat to Transfer?
Because the graft is your own fat, you need a donor supply, and this is where very lean patients meet a limit. Fat transfer is not a weight-loss operation, and the amount safely available from your abdomen, flanks, or thighs sets a ceiling on how much can be moved. Once expected resorption is subtracted, a slim frame may simply not yield enough to reach a large goal in one session. This does not rule you out, but it shapes the plan toward realistic volumes, careful harvesting of what you have, and staging when the goal is ambitious. If a clinic proposes a dramatic large-volume change on a very thin patient with no mention of these limits, that is a sign the plan is built on the brochure rather than on your body.
How a Fat Graft Actually Takes
A transplanted fat cell does not arrive with its own plumbing. When your surgeon moves fat, the graft is temporarily cut off from a blood supply, and it survives at first only by absorbing oxygen and nutrients that soak in from the surrounding tissue. That window is a race. New blood vessels must grow into the graft within days, or the cells starve.
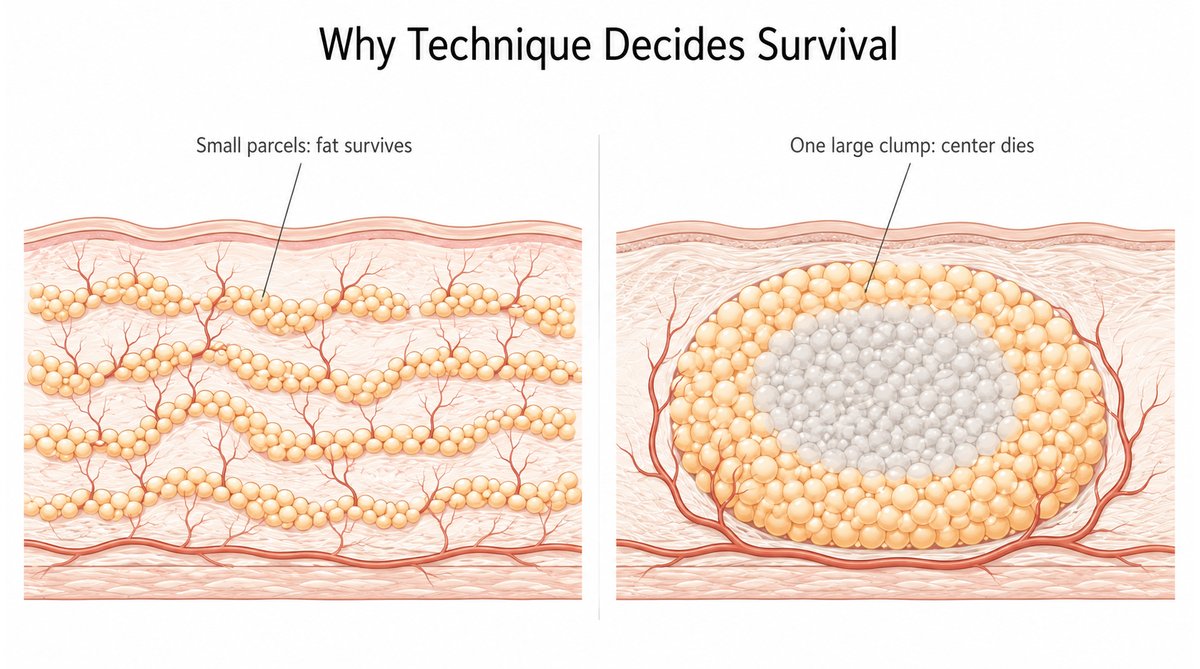
Because oxygen only diffuses a short distance, the fat at the outer edge of each deposited parcel, closest to living tissue and new vessels, tends to survive. Fat trapped in the dense center of a large clump is most likely to die. This is the entire reason technique matters so much. Fat placed in many fine threads, spread through well-supplied tissue, presents mostly edges and survives well. That same volume dumped as one big lump presents mostly center and largely dies. Reviews of fat grafting technique describe this as structural grafting: multiple passes at different depths, small aliquots, building a three-dimensional lattice that new vessels can grow into.
Surgeons often picture a graft as three zones. At the outer surface sits a thin surviving zone, fed well enough to live outright. Just inside is a regenerating zone, where some cells die but the scaffold and resident stem cells recruit new tissue. At the core of any parcel that is too large sits a necrotic zone, where everything dies and is cleared, sometimes leaving a firm nodule or an oil cyst behind. The craft of fat grafting is placing fat in parcels small enough that almost all of it falls in the first two zones and almost none in the third.

Understanding this gives you a realistic mental model. A fat graft is not a fixed object you deposit; it is living tissue asking your body to adopt it, and your body only adopts what it can feed.
How Much Actually Survives, by Area
There is no single survival number, because retention depends heavily on the recipient area, the volume, and how it was measured. Honest ranges from the published literature look like this.
Fat Graft Retention at a Glance
| Area | Reported retention | Why it lands there |
|---|---|---|
| Face, well-vascularized zones (cheeks) | Higher, often around half or more | Rich blood supply, tiny volumes, little movement |
| Face, thin zones (temple, tear trough) | Lower, roughly a third | Poor vascularity, unpredictable take |
| Breast | Roughly 40 to 50 percent at one year | Moderate supply; measured volumes vary widely by method |
| Buttock (BBL) | Often 60 to 70 percent by six months, but a wide 15 to 83 percent across studies | Large volumes, but responds well when technique and aftercare are good |
A systematic review of fat grafting survival found long-term retention commonly in the range of a third to two thirds. Early literature settled on a rough rule that only about a third of injected fat survives at one year. In the breast specifically, a systematic review of how retention is measured reported one-year retention around 36 to 47 percent depending on the imaging used, which is a useful reminder that even the numbers themselves shift with the measuring tool. In the buttock, modern three-dimensional imaging has reported retention near 78 percent at three months settling to around 65 percent at six months, while the broader literature spans a very wide range.
One reason the published numbers scatter so widely is that measuring surviving fat is genuinely hard. Different studies use calipers, three-dimensional surface scans, or MRI, and each reads volume differently, so two honest surgeons can quote different figures for the same procedure. Treat any single percentage as an estimate within a range rather than a precise guarantee, and weigh the pattern across studies over any one headline number.
Put simply: treat any promise of near-total survival with suspicion, and expect the face to reward good vascularity and punish thin, poorly supplied zones.
The Timeline: When the Loss Happens
Fat loss is not gradual and endless; it is front-loaded. Most of the resorption happens in the first three months, as the grafts that failed to gain a blood supply are cleared away. By around six months, the picture stabilizes, and the fat that is still present has established its own circulation and is, for practical purposes, permanently yours.
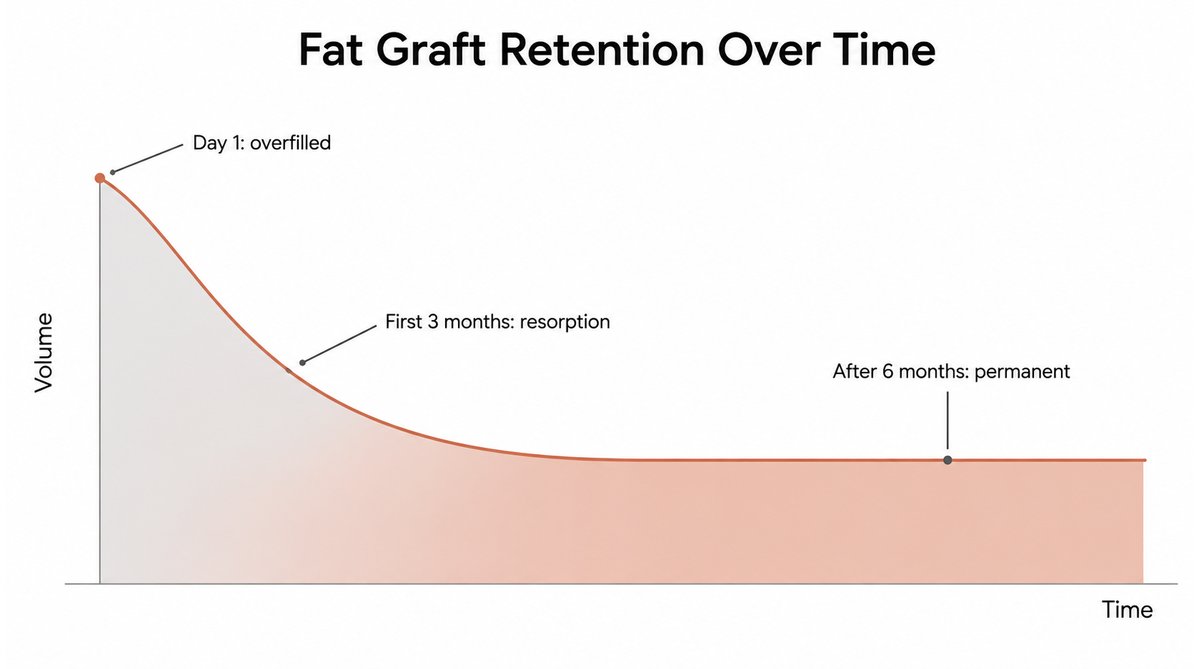
This timeline explains two things patients often misread. First, the deflation you see in the early weeks is expected and does not mean the procedure failed; it means the unsurvivable portion is leaving, exactly as planned. Second, your true result should be judged at around six months, not at six days when you are still swollen, and not at six weeks when resorption is still underway. What survives to the six-month mark tends to behave like the rest of your body fat from then on, shrinking if you lose significant weight and growing if you gain it.
What Actually Determines Survival
Retention is not luck. A handful of factors, some in your surgeon’s hands and some in yours, decide whether a graft thrives.
Recipient site blood supply
The tissue receiving the fat has to feed it. Well-vascularized areas like the cheeks hold fat better than thin, poorly supplied zones like the temple, and a recipient bed that has been scarred by radiation or previous surgery holds it worse. Your anatomy sets a ceiling that no technique fully overrides.
Harvesting and processing
Fat is fragile. Gentle, low-pressure harvesting and careful processing preserve living cells, while rough suction or overly aggressive spinning damages them, so that what is injected is partly dead on arrival. The care taken during the quiet, unglamorous middle of the operation matters as much as the injection itself.
Injection technique and volume per area
Small parcels spread through many passes survive; large boluses do not. Overfilling a space beyond what its blood supply can support does not add lasting volume, it just adds fat that will die, sometimes forming firm lumps or oil cysts. This is why a well-matched plan respects how much a given area can actually nourish.
Your own biology and habits
Smoking constricts the small vessels a graft depends on and is one of the most powerful ways to sabotage your own result. Poorly controlled diabetes and significant weight fluctuation during healing work against retention too. Younger, healthy tissue with good circulation tends to hold grafts better than tissue already compromised by these factors.
Do Stem Cells, PRP, or Cell-Enriched Fat Improve Survival?
Clinics advertise stem cell fat transfer, PRP-boosted grafting, and nanofat, all promising better survival, and the science is genuinely interesting but more mixed than the marketing suggests. Enriching a graft with stromal vascular fraction or laboratory-expanded fat-derived stem cells has, in some studies, improved retention substantially; one trial of a cell-enriched graft reported median retention around 80 percent versus about 45 percent for conventional grafting. Platelet-rich plasma has shown less consistent benefit. The honest position is that these methods are promising and still evolving, not proven shortcuts, and the words on the brochure often run ahead of the evidence. A careful, well-executed conventional graft in skilled hands still outperforms a gimmick, and no additive rescues fat that was harvested roughly or placed in tissue that cannot feed it. This survival-dependent logic is the opposite of treatments that deliver finished tissue outright rather than relying on your body to keep it, like the RE2O ECM skin booster used in the skin.
Why Your Surgeon Overfills, and When You Need More Than One Session
Because a predictable fraction of every graft will not survive, experienced surgeons deliberately overcorrect, injecting more than the final volume you want so that the surviving portion lands on target. This is not upselling; it is arithmetic applied to biology, and a surgeon who does not account for resorption will leave you undercorrected.
There is a limit to overcorrection, though. You cannot force more fat into an area than its blood supply can feed, because the excess simply dies and can create complications. When the volume you want exceeds what one session can safely nourish, the correct answer is staging: a second, and occasionally a third, session spaced months apart, each building on the surviving, now better-vascularized base of the last. A plan that promises a very large single-session change with total survival is promising something biology does not deliver. A plan that quotes realistic per-session retention and, where needed, a second session is telling you the truth.
A simple example makes the arithmetic concrete. If you want an area to gain the equivalent of 100cc of lasting volume, and realistic retention there is about half, your surgeon plans to place roughly 200cc so that the survivors add up to your target. If your goal needs 400cc of lasting volume in a space that can only safely nourish 200cc of graft at a time, no honest amount of overfilling reaches it in one sitting. The correct plan is two sessions rather than one dangerous overload.
What You Can Do to Protect Your Result
Some of the most important variables are in your hands, both before and after surgery.
Stop smoking and nicotine well before and after your procedure, because nicotine strangles the small vessels your graft is trying to grow. Keep your weight stable through the healing months, since losing weight shrinks surviving grafts and gaining it distorts them. Follow your surgeon’s instructions on pressure and positioning precisely; in a buttock graft this means the well-known restriction on sitting directly on the area during early healing, because compressing a graft before it has a blood supply crushes it. Eat and hydrate well, and avoid anything that impairs circulation during the critical first weeks. Give the graft time before judging it, because the tissue that will survive is quietly building a blood supply during exactly the weeks you are most anxious to see a result. None of this can rescue a poorly executed graft, but neglecting it can ruin a well-executed one.
Surgeon’s Insight: Plan for What Survives, Not What Goes In
The most common way patients feel let down by fat transfer is by falling in love with the day-one result. On the table and in the first days, an overcorrected area looks full, sometimes fuller than you wanted, and it is tempting to believe that is your result, but it is not. A meaningful fraction of that volume is fat that has not yet won a blood supply and will leave over the following months.
The judgment that separates a satisfying result from a disappointing one is made before the first cannula moves: reading how much a given area can truly nourish, harvesting and placing fat so the maximum survives, overcorrecting by the right amount, and staging when the goal exceeds one safe session. Plan around the fat that survives to six months, not the fat that goes in on the day, and expectation and reality finally meet.
What Fat Grafting Cannot Promise
Be wary of specific claims that biology does not support. No honest surgeon can guarantee a fixed survival percentage for you, because retention depends on your anatomy, the area, the technique, and your healing. A promise of near-total, permanent survival from a single large session is a red flag. Fat transfer also cannot lift genuinely sagging tissue or replace the structural support of an implant where large, defined projection is the goal; it adds soft volume, not a fixed scaffold. And in the buttock especially, volume is not the only consideration. Large-volume buttock fat grafting carries real, well-documented safety concerns around fat entering deep vessels, which is why buttock fat grafting safety has driven a shift toward safer, shallower, ultrasound-guided injection. A surgeon focused only on how much fat survives, and not on how safely it is placed, is optimizing the wrong thing.
Match Your Expectations to Biology, Not to the Injection Number
Fat grafting is one of the most elegant tools in body contouring, using your own tissue to soften, restore, and reshape. Its one demand is honesty about survival. Judge a plan by expected retention rather than injected volume, understand that roughly half of what goes in is a reasonable working assumption for many areas, judge your own result at six months rather than six days, and protect the graft with the habits that keep its blood supply open.
If a consultation promises you total survival, a huge single-session change, and no mention of overcorrection or staging, you have learned enough here to ask better questions. Match your expectations to how fat actually lives and dies in the body, and fat transfer becomes what it should be: a durable, natural result built from tissue your body has chosen to keep. For related reading on choosing a treatment by biology rather than trend, our guide to Rejuran, Juvelook, and Skinvive skin boosters applies the same principle to injectables.
Written by Dr. Yongwoo Lee, board-certified Korean plastic surgery specialist in facial anatomy and aesthetic procedures at VIP Plastic Surgery, South Korea.
Frequently Asked Questions About Fat Graft Survival
How much of my transferred fat will survive?
For most areas, plan on keeping somewhere around half of what is injected over the long term, though published ranges run from about a third to two thirds depending on the site, the volume, and the technique. Well-vascularized areas like the cheeks tend to hold more, thin areas like the temple less. Your surgeon overfills to account for the loss, so the surviving portion lands on your target.
When will I see my final fat transfer result?
Judge it at around six months. Most resorption happens in the first three months as the fat that did not gain a blood supply is cleared, and the picture stabilizes by roughly six months. Early deflation in the first weeks is expected and does not mean failure. Whatever survives to six months has its own circulation and is, for practical purposes, permanent.
Is the surviving fat permanent?
Largely yes. Fat that establishes a blood supply and survives past about six months behaves like the rest of your body fat from then on. That also means it responds to your weight: significant weight loss will shrink it, and weight gain will enlarge it. Keeping your weight reasonably stable is the best way to hold your result over the years.
Why does my surgeon inject more than I asked for?
Because a predictable fraction of every graft will not survive, surgeons deliberately overcorrect so that the surviving volume matches your goal. It looks overfull at first, then settles as the unsurvivable portion resorbs. Overcorrection has limits, though; forcing in more than an area can nourish just creates fat that dies and can form lumps, which is why some goals need a second session instead.
What can I do to make more fat survive?
Do not smoke or use nicotine before or after surgery, since it strangles the small vessels your graft needs. Keep your weight stable through healing, follow your surgeon’s positioning and pressure instructions exactly, and support circulation with rest, hydration, and nutrition. These habits protect a well-placed graft; they cannot rescue a poorly placed one.
Will I need more than one session?
Sometimes. When the volume you want is more than one session can safely nourish, staging a second session months later is the correct approach, each one building on the surviving base of the last. This is common and expected for larger goals. Be cautious of any plan that promises a very large change in a single session with near-total survival, because biology does not reliably deliver that.
How long does fat transfer last?
Once fat survives past about six months, it is essentially permanent, because it has grown its own blood supply and behaves like the rest of your body fat. It lasts for years rather than expiring on a schedule the way a filler does. The one caveat is weight: the surviving fat rises and falls with your body, so significant weight change will enlarge or shrink your result over time.
How much fat survives in a BBL versus the breast?
Both fall in broad, overlapping ranges. Buttock grafts often retain around 60 to 70 percent by six months in modern series, though studies report anywhere from 15 to 83 percent. Breast grafts commonly retain around 40 to 50 percent at one year. Technique, the volume placed, and how survival is measured explain much of the spread, so treat these as planning estimates rather than guarantees.
Does the fat come back to the area it was taken from?
No. The fat cells removed by liposuction for the graft are gone from the donor area for good and do not regrow there. If you gain weight later, the fat cells that remain throughout your body can enlarge, including near the donor site, but the harvested cells do not return. Keeping your weight stable protects both your new contour and the fat you paid to move.
Can a fat transfer fail completely?
Total loss is uncommon with good technique, but rough harvesting, overpacking an area beyond its blood supply, smoking, or heavy pressure on a fresh graft can cause most of it to resorb. Partial loss is normal and planned for, so a near-total loss usually points to a technique or aftercare problem rather than bad luck. An experienced surgeon and careful aftercare are your best protection.
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified medical professional before making any decisions about surgical or non-surgical procedures.