
The Choice Almost Every Double Eyelid Patient Gets Backwards
Most people walk into a double eyelid consultation having already picked a method. They have read that the non-incisional technique means less swelling and no scar, so they want that one. Or they have read that incisional lasts longer, so they want that one instead. Both are choosing the answer before anyone has looked at the actual problem, which is the single most common reason a double eyelid fails and needs revision later.
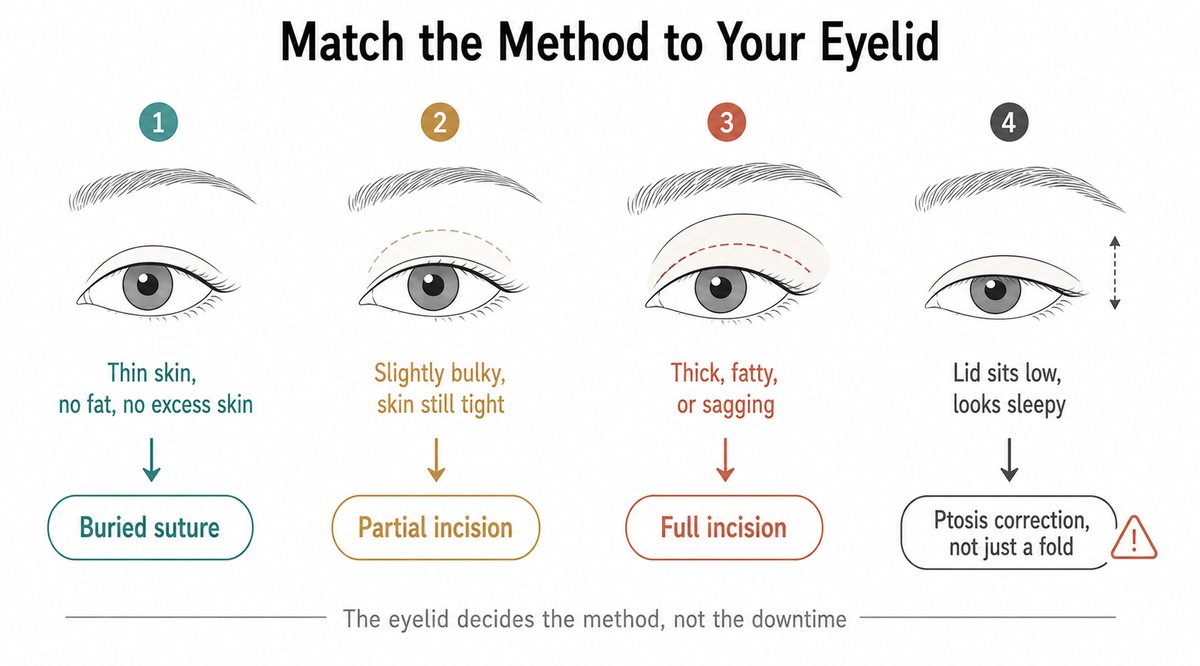
The short answer: your eyelid decides the method, not your preference. A non-incisional (buried suture) technique creates a fold with stitches alone and removes nothing, so it suits thin, light eyelids with no excess skin. An incisional technique opens the crease so a surgeon can remove skin, muscle, and fat, which is what a thick, heavy, or sagging eyelid actually needs. A partial incision sits between the two. Choose against your anatomy and the fold either loosens or turns thick and puffy.
This guide explains how a crease is actually held in place, what each of the three techniques can and cannot do, which eyelid belongs to which method, and the one condition that quietly ruins results when it is missed.
The Real Question Is Not the Method, It Is Your Eyelid
Patients frame this as incisional versus non-incisional, as if one is modern and the other is old, or one is premium and the other is budget. That framing is wrong. These are not competing products. They are different amounts of surgery, and the right amount depends on how much tissue is standing between you and a clean fold.
Think of it as a spectrum rather than a rivalry. At one end, stitches alone create an adhesion and nothing is removed. At the other end, the eyelid is opened so excess tissue can be taken out before the adhesion is made. Ask one question: does your eyelid have anything that needs removing? If it does not, the light method works beautifully. If it does, no amount of clever suturing will compensate.
How a Double Eyelid Crease Actually Forms
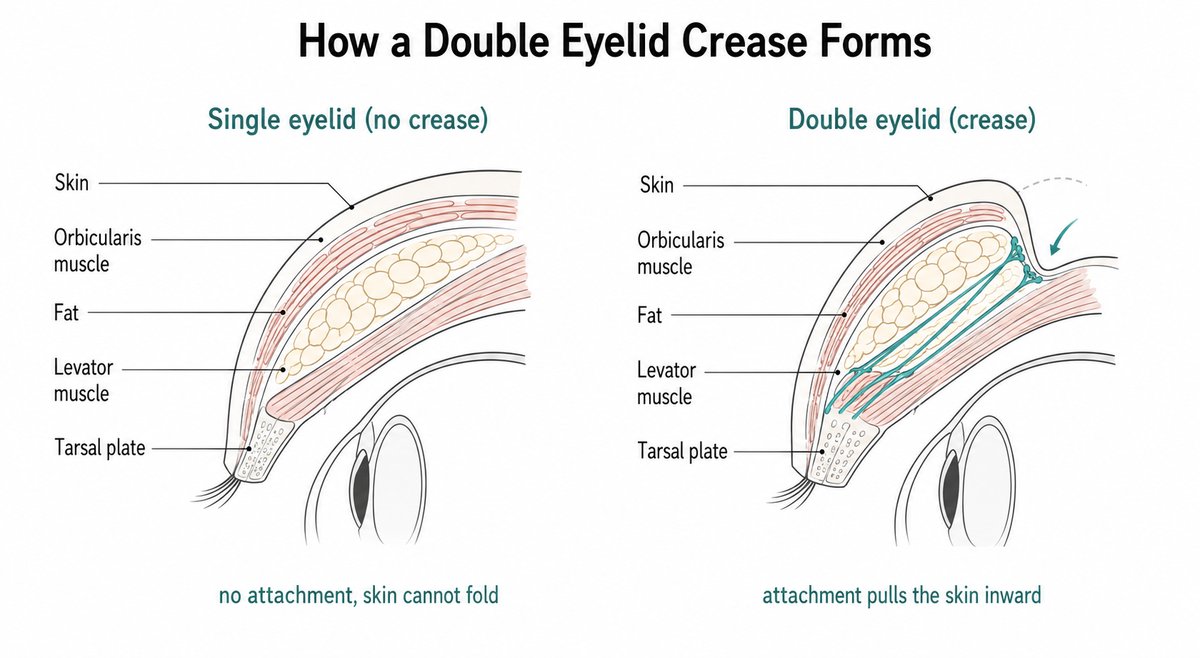
A natural double eyelid exists because the levator muscle, the muscle that lifts your lid, sends fibrous extensions forward that attach to the skin. When you open your eye, the muscle pulls and the skin at that attachment line tucks inward, producing the crease. People born without a visible crease usually lack that firm connection, or they carry enough fat and thick tissue in front of it that the skin cannot fold inward cleanly.
Every double eyelid operation, whatever the name, does the same thing: it creates an adhesion between the deep layer that moves and the skin that should fold. Techniques differ only in how that adhesion is made and whether anything is cleared out of the way first. Once you see that, the entire debate becomes simple. Stitches make the adhesion. An incision makes the adhesion and clears the obstacles.
Three Techniques, One Spectrum
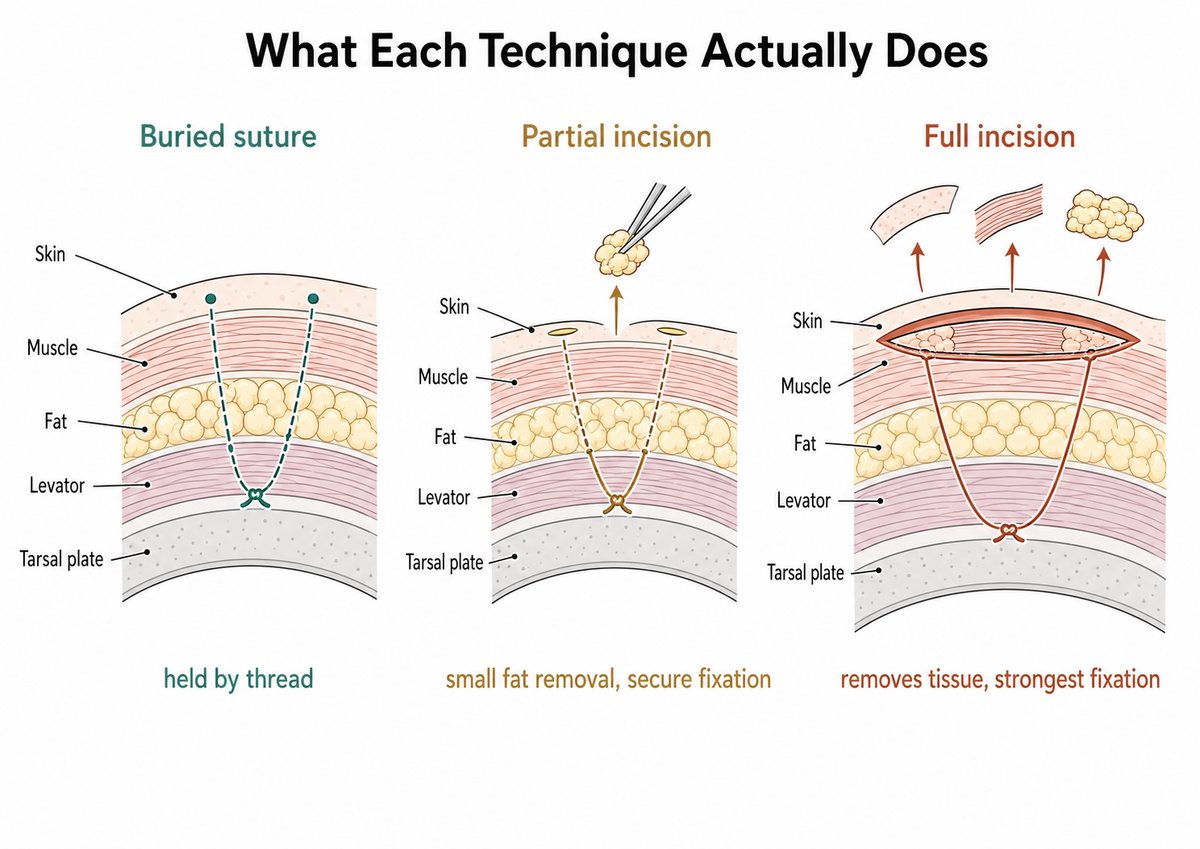
Non-incisional (buried suture)
Fine sutures are passed through tiny puncture points to anchor the skin to the deep layer, and the knots are buried under the surface. Nothing is cut open and nothing is removed. Because the tissue is barely disturbed, there is less trauma, less damage to blood vessels and lymphatics, less swelling, and no visible scar, and the result is comparatively easy to undo or repair if you dislike it.
Its limitation is structural, not cosmetic. Thread alone holds the fold. If the eyelid is thick, heavy with fat, or carrying loose skin above the crease, that thread is asked to hold weight it was never designed to hold. Over months or years, the attachment can stretch and the crease fades. Older three-point suture designs in particular carry a high recurrence rate when the skin-to-tarsus attachment is insufficient.
Partial incision
A few small openings, often only a couple of millimeters each, allow a surgeon to remove a modest amount of fat and pretarsal tissue and to fix the crease more securely, without a long incision or a large skin excision. It is the middle setting on the dial. Systematic reviews of small-incision techniques report durable, natural creases with fast recovery and no visible scar, which makes it a sensible option when the eyelid is slightly bulky but the skin is still tight.
One disclosure, since you deserve it: I do not use the partial incision. The tissue you can genuinely clear through a few small windows lands in an awkward middle, more than a suture can cope with but less than a truly bulky lid needs, so for most eyelids the honest answer sits at one end of the spectrum rather than in the middle of it. Those small openings also make it hard to place the fixation described in the next section, which engages the orbicularis, the levator aponeurosis, and the tarsus together. Other surgeons use the technique well and publish good results with it. It simply is not where the decision usually lands.
Full incision
Here the crease line is opened, so a surgeon can remove excess skin, partially thin the orbicularis muscle, and take out the fat that is blocking the fold before fixing the crease directly to the deep layer. This produces the strongest and most durable adhesion, and it is the only route when tissue genuinely has to leave the eyelid. Clearing pretarsal tissue is precisely what improves the durability of the fold and minimizes recurrence.
Its price is honest and predictable: more swelling, a longer settling period, and a scar. That scar sits inside the crease and becomes essentially invisible once healed, but it exists.
At a Glance
| Non-incisional (suture) | Partial incision | Full incision | |
|---|---|---|---|
| Tissue removed | None | Small amounts of fat | Skin, partial muscle, fat as needed |
| Holds the fold by | Buried threads | Threads plus small fixation | Direct deep fixation |
| Best for | Thin, light lids, no excess skin | Slightly bulky lids, tight skin | Thick, fatty, or sagging lids |
| Durability | Good if well selected, can loosen | Reliable | Strongest |
| Swelling | Least | Moderate | Most |
| Scar | None visible | None visible | Hidden in the crease |
| Reversibility | Easiest to undo | Limited | Permanent |
Method Is One Decision. The Crease Design Is Another.
Choosing incisional or non-incisional settles how the fold gets built. It says nothing about what the fold will look like, and that is a separate conversation you should be having. Two variables decide the look: how high the crease sits, and what shape it takes at the inner corner.
Height is the quieter of the two and the more punishing to get wrong. A crease set higher than your anatomy supports is the classic route to a thick, permanently swollen fold. It is the first thing worth arguing about and the last thing worth rushing.
Shape is what most people actually mean when they talk about a line, and three designs cover nearly everything.
In-fold
The crease runs into the epicanthal fold at the inner corner and tucks away beneath it, so the fold is narrow toward the nose and widens outward. It reads as the softest and most natural of the three, and it is usually the safest choice when the epicanthal fold is prominent, because it works with that fold instead of fighting it.
Out-fold
The crease passes outside the epicanthal fold and stays visible all the way to the inner corner, which gives a larger, more defined eye. The catch is anatomical rather than aesthetic. A prominent epicanthal fold restricts the out-fold, and forcing one on top of a strong fold tends to look unnatural or to collapse back into an in-fold over time.
Parallel
The crease runs roughly parallel to the lash line across the whole lid, the most defined of the three. It asks the most of the anatomy, and it is the design that most often depends on the inner corner being opened, because a parallel line cannot sit cleanly on top of a heavy epicanthal fold.
Why the inner corner decides what is possible
Most Asian eyelids carry an epicanthal fold, a small web of skin covering the inner corner. It is not a flaw. It is, however, the boundary of what a crease can do, which is why epicanthoplasty is treated as part of the core operation rather than an optional extra whenever an out-fold or a parallel design is the goal.
An epicanthoplasty is worth adding when the fold is prominent enough that opening it meaningfully improves the result, and it is not worth adding as a default. If your anatomy suits an in-fold and you like an in-fold, there is no reason to put another operation on your eyelid.
What Actually Holds the Fold, and How I Fix It
The fixation target decides how natural the fold looks
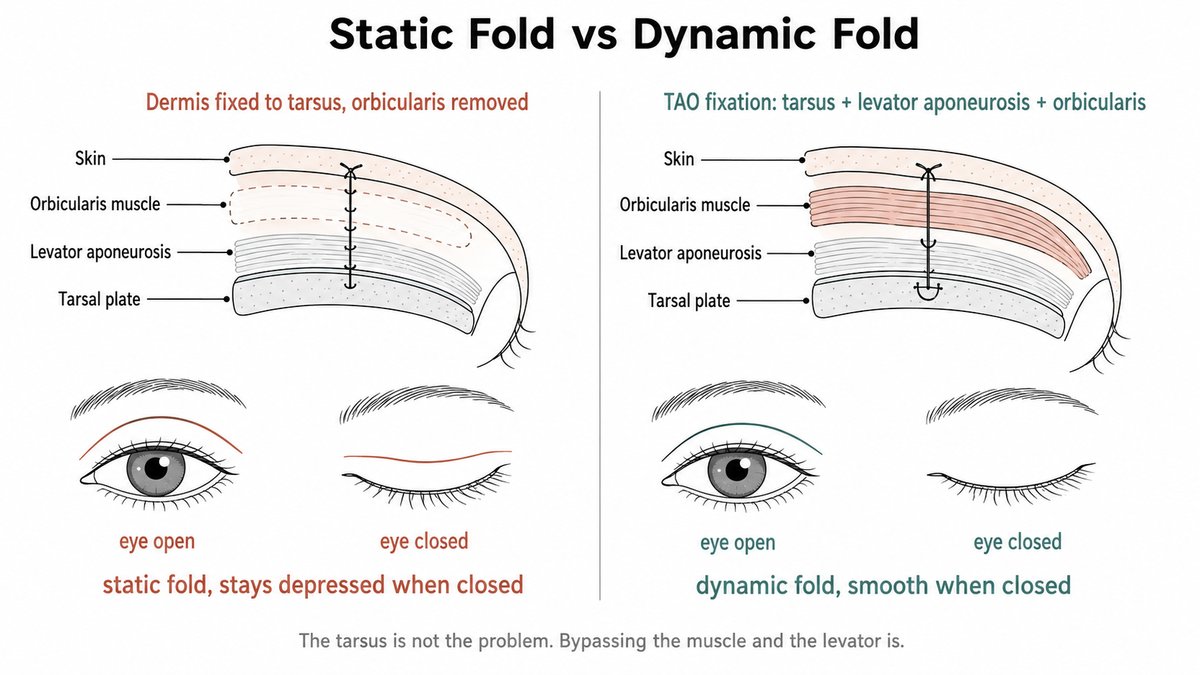
The principle behind every double eyelid operation is the same: you connect the eyelid skin, the anterior lamella, to the tissue that actually opens the eye, the levator component. An incision does it after clearing tissue out of the way, and a buried suture does it with thread alone, but the goal does not change. What does change, and what shows on your face, is which tissue that connection genuinely engages. Fixing the dermis straight to the tarsal plate, especially once the pretarsal orbicularis has been excised, produces what surgeons call a static fold: a deep, immobile line that stays visibly depressed even when the eye is closed. It is durable, and it is also one of the tells people read as operated. That overdepression tends to grow more obvious with age.
Note carefully what the problem is not. Touching the tarsus is not the error, and the fixation I use takes a partial bite of it. The error is bypassing the muscle and the levator, so the fold ends up bonded to a fixed point with no dynamic link to the tissue that opens your eye.
A fold that keeps that link behaves differently. When the fixation engages the levator aponeurosis together with the pretarsal orbicularis, the crease deepens as the eye opens and lies smooth and flat when the eye closes. Surgeons call that a dynamic fold, and it is what a physiologically natural crease does. It is the difference between a crease that moves with you and a crease that is drawn on you.
Why I use TAO fixation
My preference is to anchor the tarsus, the levator aponeurosis, and the orbicularis oculi muscle together, a fixation abbreviated as TAO. Recruiting the bulky pretarsal orbicularis rather than skin alone creates a more solid connection between the skin and the levator aponeurosis, with a significantly lower rate of relapse. Because the suture then sits perpendicular to both the aponeurosis and the muscle, the pull that blinking exerts on the fixation point is spread rather than concentrated, which is what keeps the fold from loosening over the years.
Put plainly, the fold is not hanging from your skin. It is connected to the machinery that moves your eyelid, which is how a natural crease works in the first place.
How I place the buried sutures
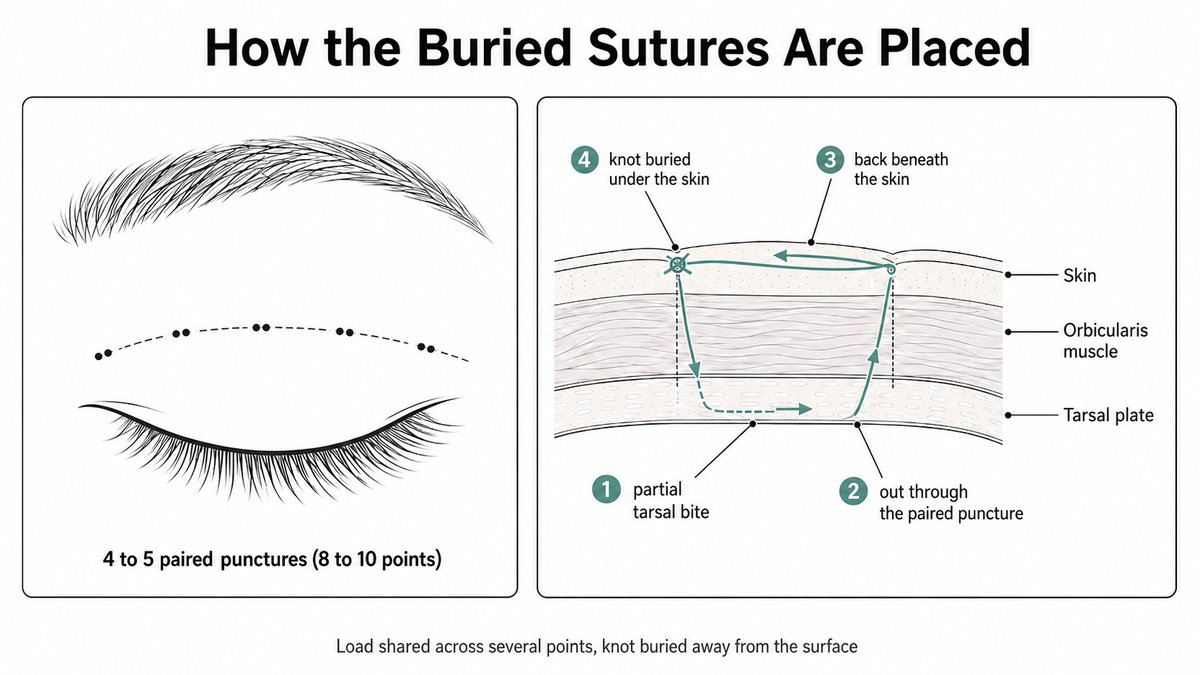
For a non-incisional case, I use four to five pairs of puncture points, eight to ten punctures in total, with the two points of each pair set close together. The suture takes a partial bite of the tarsus, passes out through the neighboring puncture, re-enters, then travels back beneath the skin to the original puncture, where the knot is tied and buried below the surface.
Two details in that description matter to you. Load is shared across several fixation points instead of resting on one or two isolated knots, which is precisely where older three-point designs tend to give way. And the knot finishes buried under the skin rather than sitting near the surface, which is what stops it from working its way out or leaving a small palpable bump months later.
Why you are woken up during the operation
Upper eyelid surgery is done under local anesthesia with light sedation, and in my hands that means midazolam and ketamine. The sedation is deliberately kept shallow enough that you can be woken partway through the operation and asked to open your eyes.
That is not a courtesy. A double eyelid only proves itself in motion. A crease that looks correct on a closed, sedated lid can sit too high or pull unevenly the moment the levator actually fires, and the only way to know is to have you open your eyes on the table and look. Checking the fold in action, then adjusting before the operation ends, is how the line drawn on your skin becomes the fold you see in the mirror.
What the Suture Method Can and Cannot Do
Non-incisional surgery has a reputation problem in both directions. Some clinics sell it as a lighter, safer, smarter version of the same operation, which is misleading. Others dismiss it as a temporary fix, which is equally wrong. It is an excellent operation on the right eyelid and a poor one on the wrong eyelid, and the difference is anatomy.
It works when the skin is thin, the eyelid is not fatty, there is no meaningful excess skin, and the levator muscle is strong. In that eyelid, the thread only has to hold a light curtain, and it does so for years. It fails when it is asked to hold a heavy one. A thick, fat-laden lid pushed into a crease by stitches alone tends either to lose the crease as the threads give way, or to bunch into a fold that stays permanently swollen and rounded. That second outcome is the thick, puffy fold patients call a sausage eye, and it is one of the most common reasons for revision surgery.
Choosing the suture method because it has less downtime, when the eyelid needed tissue removed, is not a shortcut. It is a delay.
Which Method Is Right for You: Patient Profiles
These are the cases seen most often. Find the one closest to your eyelid and take it into consultation as a working hypothesis rather than a demand.
1. Thin skin, no puffiness, no excess skin, and you are young
Your eyelid is light. There is no obvious fat bulge, the skin above the crease is not hanging, and your eye opens strongly. This is the ideal suture eyelid. A buried suture creates a clean fold, the swelling settles quickly, there is no scar, and if you ever want it changed, undoing it is straightforward. Choosing a full incision here would mean removing tissue you do not have to spare.
2. Your eyelid looks thick, heavy, or puffy
Your lid has a full, padded quality even without a crease, and pressing gently gives a soft, fatty feel. This is a debulking problem, not a stitching problem. Threads pushed through a heavy lid will either fail or produce a thick, swollen fold. An incisional approach, full or partial depending on how much bulk there is, lets the surgeon remove the fat and pretarsal tissue that is physically preventing the skin from folding.
3. Your upper eyelid skin is starting to sag or hood
Skin above your crease droops over the lash line, or you notice it resting on your lashes when you look straight ahead. Skin that is already in excess cannot be tucked away by a stitch. It has to be removed, and only an incision can remove it. Attempting a suture method here typically produces a crease that disappears under the overhanging skin within a year.
If the heaviness is actually coming from your brow rather than your eyelid, that is a different operation entirely, and our guide to sub-brow lift versus upper blepharoplasty explains how to tell the two apart.
4. Your eyes look sleepy, and the fold is not the real problem
One eye seems smaller, your upper lid sits low over the iris, you raise your eyebrows to see properly, or people say you look tired. This may be ptosis, a weak levator muscle, and it is the single most important thing to catch before surgery. Ptosis is a lifting problem, not a folding problem. Creating a crease on a lid that cannot lift itself gives you a fold that looks puffy and an eye that still looks sleepy, and it is why ptosis is treated as an exclusion for a simple fold operation. That muscle has to be addressed, which usually means an incisional approach.
5. You want the least downtime and the option to change your mind
You have an event coming, you are nervous about committing, or you simply want to try the look. If your anatomy fits profile one, the suture method is a legitimate answer to this. If it does not, the honest answer is that no method gives you a good result quickly, and rushing the choice is how people end up in revision surgery, which is far harder than the original operation.
6. You are somewhere in between
Your lid is slightly bulky, the skin is still tight, and you want durability without a full incision. A partial incision is designed for exactly this case, and some surgeons will offer it. In practice the decision still resolves to one end of the spectrum. If the bulk is genuinely modest and the skin is tight, a buried suture with a solid TAO fixation holds well. If the bulk is enough to fight the fold, an incision that actually clears it is the more honest answer. Ask your surgeon which side of that line your eyelid falls on, because being somewhere in between describes your eyelid, not a plan.
Recovery, Scars, and How Long It Looks Unnatural
Expect the timeline to track the amount of surgery, because that is all it reflects. With a suture method, most of the visible swelling settles within roughly one to two weeks, and the fold keeps softening for a few months. With a full incision, the swelling is more pronounced and takes several weeks to subside, and the crease continues to relax and look more natural over three to six months. A partial incision sits between them.
Skin sutures come out about a week after an incisional operation, and most people are presentable enough to return to work once they are out. A buried suture case is usually quicker than that. Eye makeup waits longer than people expect, generally until around the two week mark, once the incision has sealed fully.
Two things are worth saying plainly. First, every fresh double eyelid looks too high and too thick at the beginning. That is swelling, not the result, and judging your outcome in the first month is the fastest way to make yourself miserable. Second, the incision scar is a real scar, but it lies within the crease, and by the time the fold has settled it is not something other people see.
Surgeon’s Insight: Match the Method to the Eyelid, Not to the Downtime
Almost every unhappy double eyelid I revise was not a technical failure. It was a selection failure. Someone with a thick, fatty lid was given stitches because stitches sounded easier, and the fold either vanished or turned into a swollen sausage. Someone with an unrecognized ptosis was given a crease when what they needed was a muscle corrected. Each operation was performed competently. It was simply the wrong operation.
This decision belongs to your anatomy, and anatomy is not a matter of opinion. A surgeon should be able to tell you, by looking at and touching your eyelid, how thick the skin is, how much fat sits behind it, whether there is excess skin, and how strongly the levator lifts. If those four answers are not part of the conversation, you are not choosing a method. You are guessing.
Safety, Risks, and What to Watch For
Both routes are safe in trained hands, and the risks are mostly the kind that resolve. Swelling, bruising, mild asymmetry in the early weeks, and a fold that sits higher than its final position are all expected and settle.
Specific risks differ by method. A suture technique can produce suture-related complications, such as a knot working its way toward the surface, small cysts along the line, or, uncommonly, a stitch irritating the eye itself, which needs prompt attention rather than patience. Its most common problem, though, is simply loss of the crease over time when the eyelid was too heavy for it. An incisional technique carries the ordinary risks of an open procedure: a scar, more swelling, and a small chance of asymmetry that needs adjusting.
One risk matters more than any of these: a missed diagnosis. An eyelid with ptosis, significant excess skin, or a heavy fat pad that is treated as a simple fold will produce a disappointing result no matter how skillfully the chosen technique is executed. Ask what your surgeon found, not just what they plan to do.
Match the Method to Your Eyelid, Not to the Trend
Incisional and non-incisional are not rival philosophies. They are different amounts of the same operation. Stitches alone suit a thin, light eyelid with nothing to remove. A partial incision suits a slightly bulky lid with tight skin. A full incision is necessary when skin, muscle, or fat genuinely has to leave the eyelid, and when a weak levator has to be corrected at the same time.
If you take one thing from this, take the diagnostic question rather than the method. How thick is my skin, how much fat is behind it, do I have excess skin, and how strongly does my eyelid lift? A surgeon who answers those four before naming a technique is choosing for your eyes. A clinic that names the technique first, especially the one with the shortest downtime, is choosing for their schedule.
Written by Dr. Yongwoo Lee, board-certified Korean plastic surgery specialist in facial anatomy and aesthetic procedures at VIP Plastic Surgery, South Korea.
Frequently Asked Questions About Incisional and Non-Incisional Double Eyelid Surgery
What is the difference between incisional and non-incisional double eyelid surgery?
Non-incisional surgery creates the crease with buried stitches and removes nothing, so it causes little swelling and leaves no visible scar. Incisional surgery opens the crease so the surgeon can remove excess skin, muscle, and fat before fixing the fold directly, which is stronger and more durable. Which one is right depends on whether your eyelid has tissue that needs removing.
What is a dynamic double eyelid fold?
A dynamic fold deepens when you open your eye and flattens smoothly when you close it, which is how a natural crease behaves. It happens when the fixation engages the levator aponeurosis and the pretarsal orbicularis muscle rather than anchoring skin to the tarsus alone. A fold that stays visible and indented on a closed eye is the version people tend to read as operated.
What is TAO fixation in double eyelid surgery?
TAO means fixing the tarsus, the levator aponeurosis, and the orbicularis oculi muscle together, rather than relying on skin-to-tarsus fixation alone. Recruiting the pretarsal orbicularis gives a more solid connection to the muscle that lifts the lid, spreads the pull of blinking across the fixation, and is associated with a lower rate of the fold loosening over time.
What is the difference between in-fold, out-fold, and parallel double eyelids?
An in-fold crease tucks into the epicanthal fold at the inner corner, so the fold is narrow toward the nose and widens outward, which reads as the softest and most natural. An out-fold stays visible past the inner corner for a larger, more defined eye. A parallel crease runs level with the lash line across the whole lid and is the most defined of the three.
Do I need an epicanthoplasty with my double eyelid surgery?
Only if your inner corner requires it. A prominent epicanthal fold physically restricts an out-fold or a parallel crease, so those designs often need the corner opened to sit cleanly. If your anatomy suits an in-fold and you are happy with an in-fold, there is no reason to add the operation. It is worth doing when it meaningfully improves the result, not by default.
Are you awake during double eyelid surgery?
The operation is done under local anesthesia with light sedation, and you are woken partway through and asked to open your eyes. That is deliberate. A crease that looks right on a closed, sedated lid can sit too high or pull unevenly once the eye actually opens, so checking the fold in motion on the table is the only reliable way to confirm the design before finishing.
When can I wear eye makeup and go back to work?
Skin sutures come out about a week after an incisional operation, and most people are presentable enough to return to work once they are out. A buried suture case is usually quicker. Eye makeup waits longer than most people expect, generally until around two weeks, once the incision has sealed fully.
Which method lasts longer?
A full incision holds the longest, because the fold is fixed directly to the deep layer after the obstructing tissue is removed. A well-selected suture method can also last for many years, but it loosens more often when it is used on a thick, fatty, or sagging eyelid that was never suitable for it. Durability is decided by selection more than by technique.
Can I get non-incisional surgery if my eyelids are thick?
Usually not, and this is the most common mistake patients make. A thick or fatty eyelid physically blocks the skin from folding, and stitches cannot remove that obstacle. Forcing a crease anyway tends to produce either a fold that fades or a thick, permanently puffy fold. That eyelid needs the fat and pretarsal tissue removed, which requires an incision.
Does non-incisional double eyelid surgery leave a scar?
No visible one. Threads pass through tiny puncture points that heal without a noticeable mark, which is one of its genuine advantages. A full incision does leave a scar, but it sits within the crease itself, and once the fold has settled over several months it is not something other people notice.
How long is the recovery for each method?
With the suture method, most visible swelling settles in about one to two weeks. With a full incision, the swelling is heavier and takes several weeks, and the fold keeps relaxing and looking more natural over three to six months. A partial incision falls in between. Every fresh crease looks too high and too thick at first, and that is swelling rather than your result.
Is non-incisional surgery reversible?
It is the easiest of the three to undo or adjust, because nothing was removed and the fold is held by threads that can be released. That said, reversible does not mean consequence-free, and repeated operations on the same eyelid build scar tissue that makes future surgery harder. It is a reason to choose carefully, not a reason to choose casually.
What is partial incision double eyelid surgery?
It uses a few very small openings rather than one long incision, which lets the surgeon remove a modest amount of fat and fix the crease securely without a large skin excision. It suits an eyelid that is slightly bulky but still has tight skin. Recovery stays closer to the suture method while durability moves closer to the incisional one.
Can double eyelid surgery fix droopy or sleepy eyes?
Not by itself. If your upper lid sits low over the iris and you lift your brows to see, the likely problem is ptosis, a weak lifting muscle, which is separate from the crease. Making a fold on an eyelid that cannot lift leaves you with a puffy fold and an eye that still looks sleepy. That muscle itself has to be corrected, which usually means an incisional approach.
Why did my double eyelid disappear or get thicker after surgery?
Two causes are typical: a suture method used on an eyelid that was too heavy for it, so the threads gradually gave way, or a crease set too high for your anatomy, which bunches the skin into a thick, swollen fold. Both are selection problems rather than bad luck, and both are correctable, though revision is more demanding than the first operation.
How do I know which method I need?
Four answers decide it: how thick your eyelid skin is, how much fat sits behind it, whether you have excess skin, and how strongly your levator muscle lifts. A surgeon should establish those by examining and touching your eyelid before naming any technique. If a method is recommended before those four are assessed, the recommendation is not based on your eyes.
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified medical professional before making any decisions about surgical or non-surgical procedures.