Table of Contents
The Mistake Almost Every Overfilled Patient Makes
Someone looks in the mirror, decides their face has become heavy, wide, or somehow not theirs anymore, and reaches one of two conclusions. Either the filler has worn off and they need more of it, or the filler ruined their face and dissolving it will give them back the face they had. Both conclusions are wrong, and they are wrong for the same reason: they assume filler is temporary and reversible. It is neither.
The short answer, and it is uncomfortable. Your filler is probably still there, even the filler from years ago. Dissolving it will not restore your old face, because what dissolving does is remove the padding that was hiding what your face actually looks like now. And if the face underneath has descended, no amount of filler and no amount of dissolving will lift it. Only surgery does that.
For a heavily filled face, the honest answer is usually not dissolve or lift. It is dissolve the filler, then lift, in that order, and the order is not a preference. It is the whole point. This guide covers how long filler actually lasts, what an overfilled face is doing mechanically, when to dissolve filler and when to operate, and why doing them in the wrong order wastes the operation.
The Real Question Is Not Dissolve or Lift. It Is What Your Filler Was Doing.
Filler adds volume. That is the entirety of what it does. It does not lift, it does not tighten, and it does not reattach anything that has come loose. When a face is injected year after year, the filler is very often being asked to do something it was never designed to do: to compensate for tissue that is descending.
That compensation works for a while, and it works in a specific and misleading way. Descent creates hollows and shadows, filler erases hollows and shadows, and the face looks better in photographs. What has not changed is the descent. Underneath, the tissue keeps sliding, and the response is more filler, and the face keeps getting heavier without ever getting lifted.
So before you ask whether to dissolve, ask what the filler was covering. If it was covering a genuine volume deficit, filler was the right tool and you may simply have had too much of it. If it was covering descent, filler was the wrong tool from the beginning, and dissolving it will not solve the problem. It will only make the problem visible.
Why Your Filler Did Not Go Away
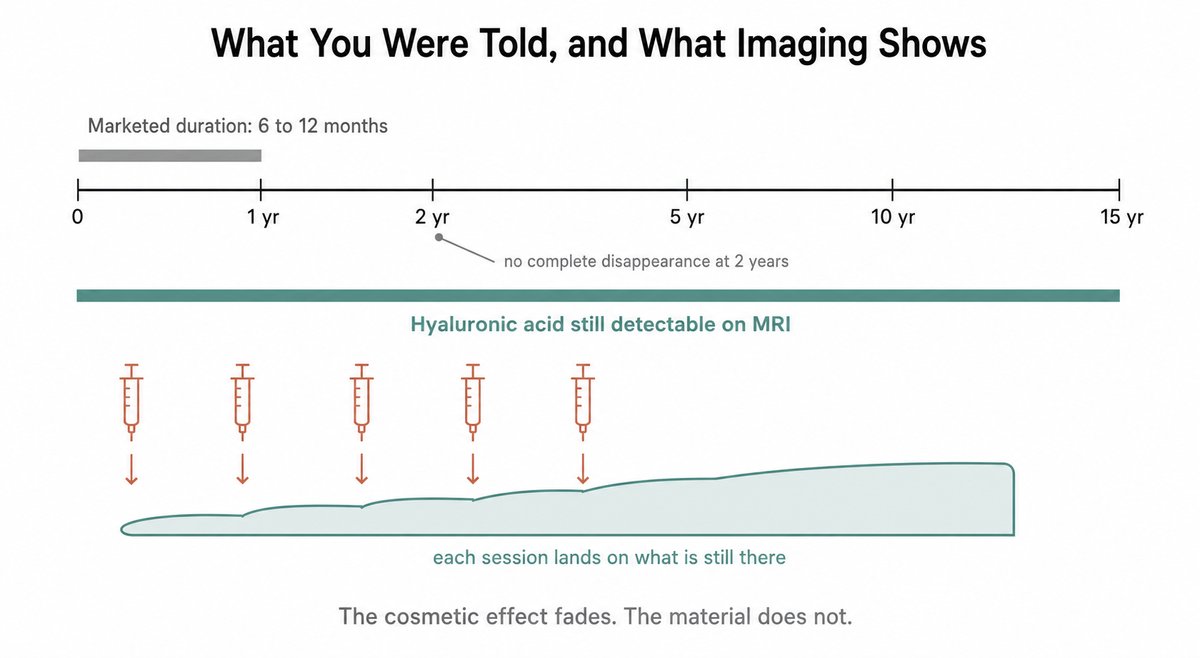
Hyaluronic acid filler is sold as lasting six to twelve months. Imaging says otherwise, and the gap between those two statements is the single most important thing to understand about an overfilled face.
A review of magnetic resonance imaging studies in the mid-face found hyaluronic acid still present in every patient scanned, with no complete disappearance over a two year window, and filler still detectable in some patients eight to fifteen years after injection. Not a trace. Detectable volume. Individual case reports have made the same point from the clinical side, with filler behaving as a live presence in tissue years after everyone assumed it had gone.
What fades is the cosmetic effect, not the material. Filler integrates into the tissue, spreads, compresses, and shifts away from where it was placed. It stops holding a crisp contour, so the face looks like the filler is gone, and another syringe goes in on top of the filler that never left. Do that twice a year for six years and the arithmetic stops being about how long filler lasts. It becomes about how much filler is now in your face.
Accumulation, not any single bad injection, is the mechanism behind almost every overfilled face I see. Nobody decided to overfill. Each individual session was reasonable. What was unreasonable was the assumption underneath all of them, which is that the slate had been wiped clean since the last one.
How a Face Becomes Overfilled
Overfilled faces are not simply faces with too many milliliters in them. A clinical review of facial overfilled syndrome describes three mechanisms working together, and recognizing which one is dominant in your face changes what should be done about it.
The first is a volume mismatch. Filler is placed in a compartment that cannot hold that much, so it does not build the contour it was meant to build. It bulges, it spreads into neighboring compartments, and it blurs the boundaries between them. Cheeks flatten outward instead of projecting. Definition disappears. Lips are where patients notice this first and most clearly, because the spread has a name there and a shape everyone recognizes, which is filler migration and the duck lip it produces.
The second is biomechanical. Filler placed within or beneath the muscles of facial expression restricts how those muscles move, and filler placed under the skin stretches the skin envelope. A face can look acceptable at rest and wrong the moment it smiles, and that is the tell most patients notice first without being able to name it. Anatomically this is a mismatch between where the filler was delivered and what that compartment was built to hold.
The third is simply accumulation, which brings us back to the imaging: the payload of every previous session is still contributing.
There is a fourth consequence, and it is the one that decides whether surgery ends up on the table. Filler occupies space, and skin is draped over whatever occupies it. Take the filler away and that skin is suddenly surplus, because the volume it was covering is gone. On a young, elastic face much of it will recoil. On a face that has been aging underneath the filler for a decade, it will not, and what you are left looking at is skin that was in excess all along.
Your Three Options, and What Each Actually Does
Patients arrive believing they are choosing between products. They are not. They are choosing between three fundamentally different interventions, only one of which addresses descent.
Add more filler
This is what most overfilled patients are offered, and on a face that is genuinely deflated with tight skin, it is a reasonable answer. On a face that is heavy, blurred, and already carrying years of product, it is the worst available option, because it treats the visible symptom of descent by adding weight to a structure that is already failing to hold what it has.
Dissolve only
Hyaluronidase breaks down hyaluronic acid, and it works. What it does not do is restore. Dissolving reveals the face that has been underneath the filler, and patients are frequently shocked by it, because it is older and looser than the face they remember. This is not damage from the enzyme. It is the passage of time that the filler was concealing.
Dissolving is the correct and complete answer when the underlying face is still well supported. It is only half an answer when it is not.
Dissolve, then lift
A facelift repositions tissue that has descended and removes the skin that is now in excess. It is the only one of the three that addresses the actual problem in a heavily filled, heavily descended face. Doing it after dissolving rather than before is not a scheduling detail, and the reason is explained in the technique section below.
At a Glance
| More filler | Dissolve only | Dissolve, then lift | |
|---|---|---|---|
| What it treats | Volume deficit | Excess filler | Descent and excess skin |
| Effect on descent | None, and it adds weight | None | Corrected |
| Best for | Deflated face, tight skin | Overfilled face, good support | Overfilled face with laxity |
| What you look like after | Fuller, often heavier | Older than you expected | Lifted, and lighter |
| Can it be undone | Less than you were told | Only by filling again | Permanent, in the useful sense |
| Volume afterward | Excess | Often deficient | Restored with your own fat |
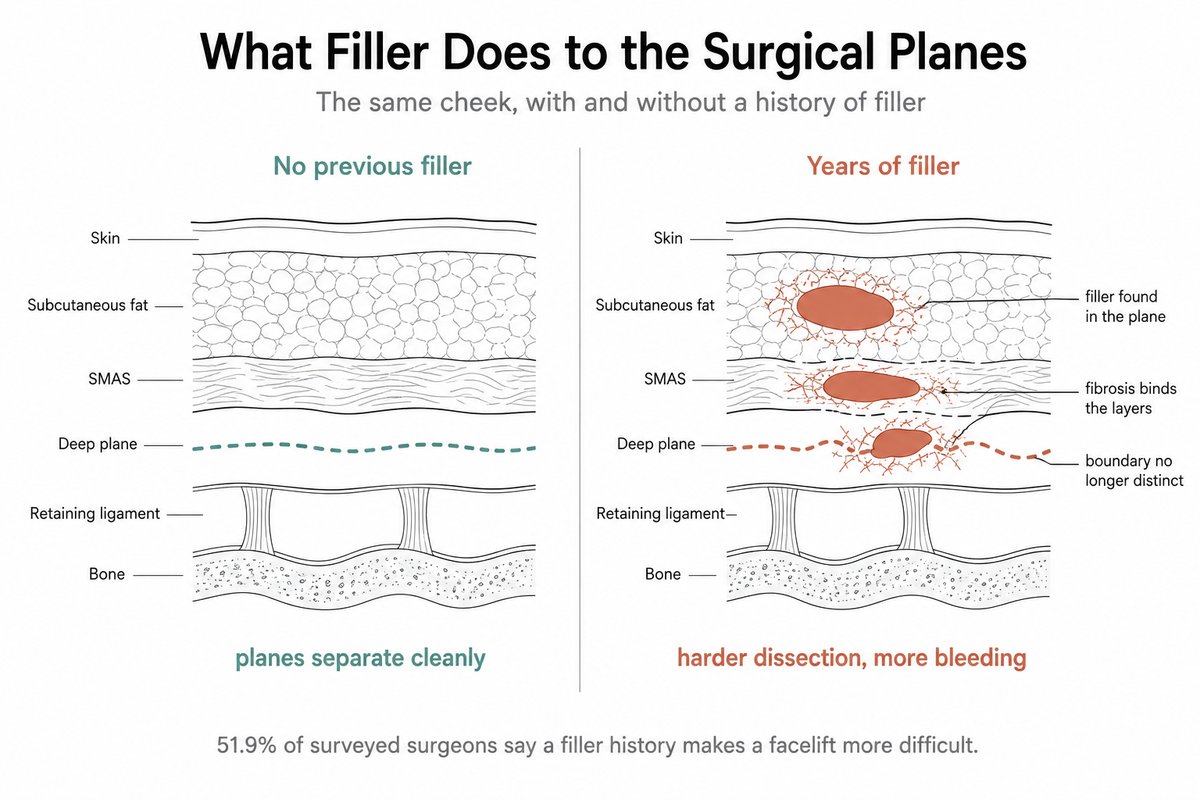
What I Actually Find When I Open a Filled Face
Filler does not politely wait to be dissolved. It is in the surgical planes.
When I lift a face that has been injected repeatedly, I encounter the filler itself during dissection in a majority of cases. Not as a memory of filler. As material, sitting in the tissue.
Around it, the tissue is fibrotic. That fibrosis is the real problem, and it changes the operation in three ways that matter to you. Dissection becomes considerably harder, because the planes that should separate cleanly are stuck together and no longer look like the planes I am trained to recognize. Risk of injuring tissue goes up, because when the planes are indistinct, the margin for error shrinks. Bleeding increases, and more bleeding means a higher chance of a hematoma, which is the most common serious complication of a facelift and the one I have written about preventing with a hemostatic net.
This is not only my impression. When members of the Aesthetic Society were surveyed about operating on patients with a history of repeated panfacial filler, 51.9 percent of the surgeons who answered said it increased the difficulty of performing a facelift, and 39.7 percent believed it raised postoperative complication rates. Asked what they had actually run into, 32.7 percent reported filler that stayed palpable or visible after surgery, 15.4 percent reported compromised blood supply to the flap, and 9.6 percent reported a lifting effect that did not last as long. Read those as what surgeons report seeing, not as the odds for any one patient. Surgeons operating on complicated fillers put it in plainer terms: dissection is difficult because of the fibrosis and granulomatous reaction.
An honest way to put this to a patient considering a first syringe: filler is not free of consequences for the operation you may want in ten years.
Why I dissolve before I operate
I inject hyaluronidase directly into the filler and dissolve it before surgery, and I ask patients to have it done if they arrive without having done it. Two reasons, and neither is cosmetic. Surgery on a dissolved face is easier, and surgery on a dissolved face is safer, for exactly the reasons above.
In practice I give an adequate dose in a single session rather than dividing it across several. Most clinicians work at a concentration of 150 units per milliliter, which is the most commonly used preparation, and the dose is adjusted to how much filler is present and how heavily cross linked it is. Dose matters more than ceremony here: more heavily cross linked fillers resist the enzyme and need more of it, and an inadequate dose is the reason patients end up being dissolved three and four times. Breakdown itself is fast, usually complete within one to three days, though the tissue takes about two weeks to settle into its final appearance.
I operate roughly two weeks after dissolving. That interval is not about the enzyme, which has long since finished its work. It is about waiting for the swelling to leave and the face to tell the truth, because I cannot plan a lift on a face that is still moving.
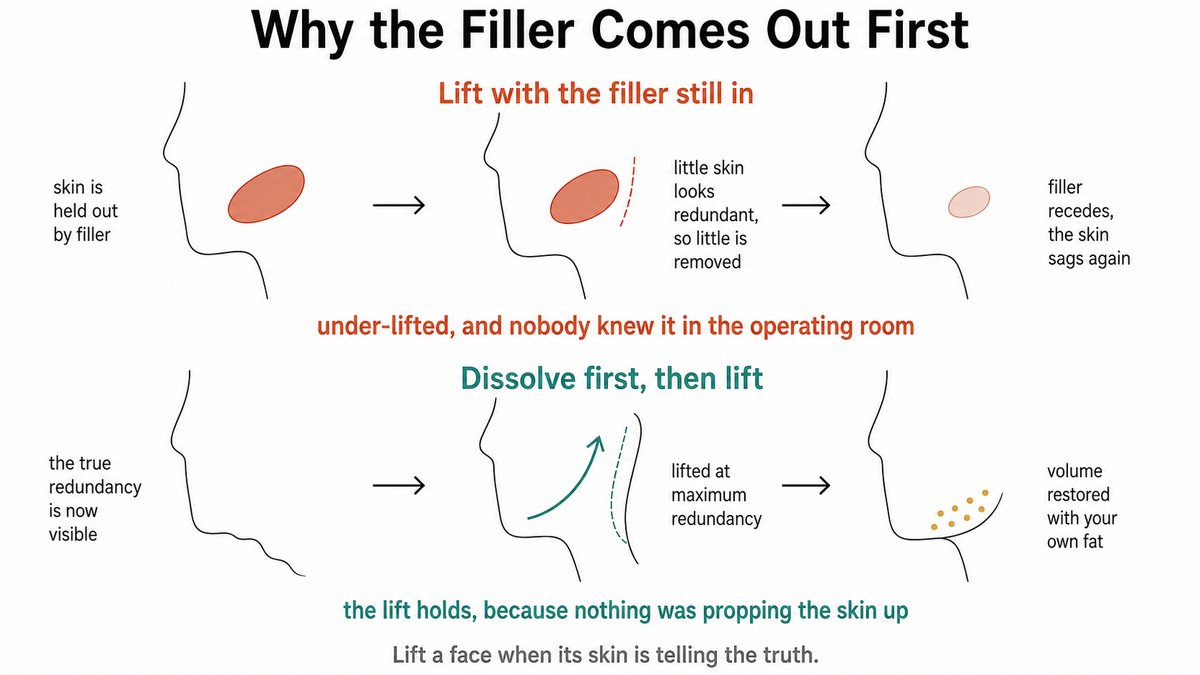
Why I do not simply lift a filled face
This is the part patients find counterintuitive, and it is the reason the order is not negotiable.
If I lift a face that is still holding filler, I am lifting a face that is being propped up. The skin is stretched over that volume, so it is not as redundant as it will be. I remove the amount of skin that appears to be in excess on that day, I close, and the result looks good. Then, over the following months and years, the filler does what filler eventually does, and the volume that was propping the skin up recedes. The skin that is left over has nowhere to go. It sags again.
I would have under-lifted, and I would not have known it in the operating room.
A face must be lifted when its skin redundancy is at maximum, and the redundancy is at maximum after the filler is gone. That is the entire argument, and it is the failure the surveyed surgeons described from the other end when they reported lifts that did not last in filler patients. Dissolving first is how you avoid being one of them.
If dissolving leaves you hollow, I fill it with your own fat, during the operation
Removing years of filler frequently leaves genuine volume deficits, and this is the reasonable fear patients have about dissolving. It is a real fear and it deserves a real answer, not reassurance.
My answer is to correct the volume during the lift, with fat grafted from the patient rather than with more product. Structure is repositioned, skin is redraped, and where the face is genuinely deficient after the filler is gone, fat is placed to fill it. Fat behaves differently from filler, does not carry the same accumulation problem, and where it survives it survives as living tissue rather than as a gel that has to be topped up. How much survives is a real question with a real answer, which I have written about in detail in how much transplanted fat actually lasts.
So the sequence is: dissolve, wait about two weeks, then lift and refill in the same operation, with your own tissue.
Which One Are You
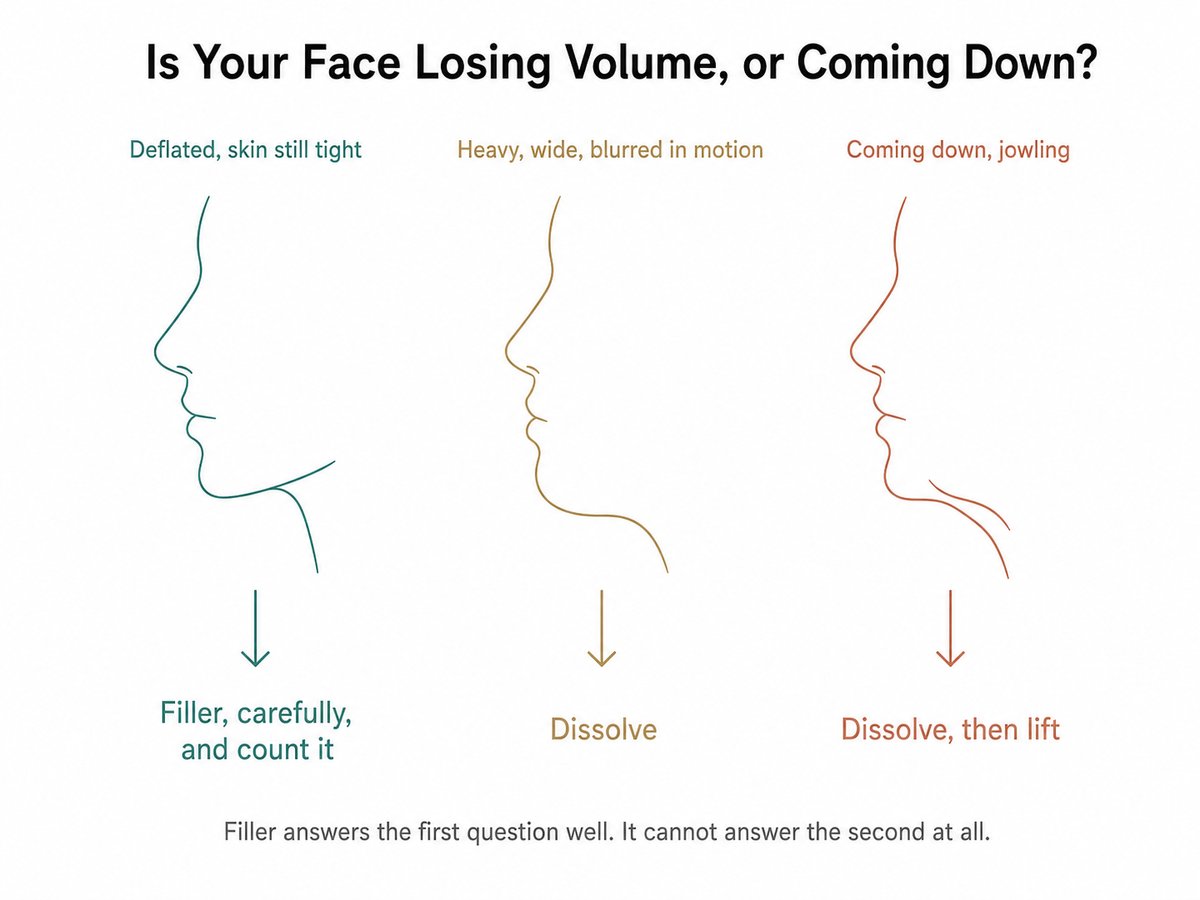
Before the profiles, the question that sorts them. A face that is deflated with tight skin has a volume problem, and filler is the right tool for it. A face that is heavy, wide and blurred in motion is holding more product than it can carry, and the answer is to take it out. A face that is coming down has a structural problem that no syringe can reach, and the answer is to take the filler out and then lift what is underneath.
1. Your face is deflated, your skin is still tight, and you are in your thirties
Volume loss is real and filler is a genuinely good tool for it. Nothing in this article says otherwise. What it says is: know how much is already in there, do not assume the last round is gone, and stop treating each syringe as if it lands on a blank face.
2. Your filler used to look good and now it does not, so you had more
Look carefully at what changed. If the shape blurred and the face widened, you are accumulating. If hollows and shadows returned, and filling them keeps working for shorter and shorter periods, you are chasing descent with a tool that cannot catch it. Second case is the one that ends in surgery, and the sooner you recognize it, the less product you will have to remove first.
3. Your face looks heavy, wide, or somehow not like you, especially when you smile
This is facial overfilled syndrome, which patients often call filler fatigue, and it is not a matter of taste. Something in your face is holding volume it cannot hold, in a compartment that cannot contain it, and restricting how your face moves. Dissolving is the starting point. Whether that is the finish line depends on what is underneath.
4. You are afraid to dissolve because you think you will look older
You will, briefly and then permanently, and I would rather say so now. What you will not become is older than you actually are. Fear here is reasonable and it is also the wrong reason to keep filling, because every year of postponement adds product that someone eventually has to remove, on a face that is descending anyway. If it helps: the volume can be put back during the lift, with your own fat, which is the section above. The truth is not optional. The hollowness is.
5. You have already dissolved, more than once, and you are unhappy with your skin
Be careful before you dissolve again. Hyaluronidase is not selective, so every round degrades your own hyaluronic acid alongside the filler, and repeated rounds are associated with hollowing around the eyes, worsening fine lines, and a deterioration in skin quality. Being dissolved four times because nobody committed to an adequate dose is worse for your tissue than being dissolved once, properly.
6. Your problem is heaviness and jowling, not volume
Then you were never a filler patient. Descent is a surgical problem, and the guides to the deep plane facelift and how it differs from a SMAS lift and to what an overtightened facelift looks like will tell you more about what that operation actually involves than another consultation about syringes will.
What Dissolving Actually Feels Like, and the Two Weeks After
Recovery from dissolving is physically minor and emotionally the hardest part of this entire article. Expect the two to be out of proportion.
Physically, it is an injection appointment. There is stinging as the enzyme goes in, then swelling and often bruising, which is worse than patients expect and can be marked around the lips and the under-eyes. Swelling peaks in the first day or two and is largely gone within a week, and the tissue reaches its true resting shape at about two weeks.
Emotionally, the difficulty arrives on a delay. For the first few days the swelling is still holding the face out, so it looks acceptable. Then the swelling leaves, and what is underneath appears, and it appears all at once. Almost everyone finds this moment distressing. Almost everyone also finds it clarifying, because it is the first accurate look at their own face in years.
Two things follow from that, and they matter more than the recovery itself. Do not make a decision in that first week, because the face is still moving and it will look worse than it is. And do not fill it again reflexively, which is the single most common reaction and the one that puts you back at the start of the cycle this article is about. Take the accurate face to a consultation. It is the only face a surgical plan can be built on.
If a lift follows, the recovery that matters is the recovery from the lift, not from the enzyme.
Surgeon’s Insight: Filler Was Never Keeping Time. It Was Hiding the Clock.
Patients tell me they have been maintaining their face for a decade. What they have often been doing is deferring a decision, and paying compound interest on it. Filler was placed to erase a shadow. Shadow came back, more filler went in. Nothing was ever lifted, and by the time I meet them there is both descent and a face full of product that makes the operation to correct the descent harder, bloodier, and less predictable than it needed to be.
I am not against filler. I am against filler used as a substitute for a diagnosis. Ask what your face is actually doing, before you ask what to put in it. If the answer is that it is losing volume, fill it, carefully, and count what you put in. If the answer is that it is coming down, no syringe in the world is going to hold it up, and every year you spend proving that to yourself is a year of product that someone eventually has to dissolve.
Safety: Dissolving Is Not Free Either
Hyaluronidase is effective, it is the correct treatment for the most feared of all filler complications, a vascular occlusion, and it saves faces. None of that makes it a neutral eraser, and the way it is marketed as a simple undo button is the second misconception this article exists to correct.
Hyaluronidase is not selective. It breaks down hyaluronic acid, and your own tissue is full of hyaluronic acid that has nothing to do with the filler. The enzyme cannot tell the difference, and it degrades your native hyaluronic acid along with the product. Reported consequences of aggressive or repeated use include hollowing around the eyes, worsening of fine lines, and deterioration in skin quality, a pattern described in the literature as posthyaluronidase syndrome. Allergic reactions are uncommon but real, and published guidelines exist precisely because dosing casually is a mistake.
There is a practical conclusion in this. Dissolving should be done deliberately, with a plan for what happens next, ideally once and adequately rather than repeatedly and timidly. A patient who has been dissolved four times because nobody committed to a dose is worse off than a patient who was dissolved once by someone who knew what they were removing and why.
And a note about what hyaluronidase cannot touch. It works on hyaluronic acid. If you have had a permanent or semipermanent filler, the enzyme will do nothing to it, and removal becomes a surgical problem, sometimes requiring the filler to be excised during the facelift itself.
Ask What Your Face Is Doing, Not What to Put In It
Filler is a volume tool. It is a good one. It is not a lift, it is not reversible in the way you were told, and it does not vanish on the schedule printed in the brochure.
If your face is deflated and your skin is holding, filler is a reasonable answer, and the only discipline required of you is to count what is already in there.
If your face is heavy, blurred, restricted when you smile, or simply not yours anymore, the filler is the thing to remove, not the thing to add.
And if what is underneath has come down, then dissolving is the first step, not the answer. Lift the face when the skin is telling the truth, restore volume with your own tissue in the same operation, and stop paying a syringe at a time for a problem that was never a volume problem.
The diagnostic question is short. Is my face losing volume, or is it coming down? A doctor who answers that before reaching for a needle is treating your face. A clinic that answers by reaching for the next syringe is treating their calendar.
Written by Dr. Yongwoo Lee, board-certified Korean plastic surgery specialist in facial anatomy and aesthetic procedures at VIP Plastic Surgery, South Korea.
Frequently Asked Questions About Overfilled Faces and Dissolving Filler
How long does hyaluronic acid filler really last?
Far longer than the six to twelve months it is sold as. A review of MRI studies of the mid-face found hyaluronic acid still detectable in every patient scanned, with no complete disappearance over a two year window and filler still visible in some patients eight to fifteen years after injection. What fades is the cosmetic effect, not the material, which is why filler accumulates in faces that are topped up on the assumption that the last round is gone.
What is facial overfilled syndrome?
It is a face that has been given more filler than its tissues can hold, producing a heavy, wide, blurred appearance that often looks worst in motion. Three mechanisms drive it: volume placed in a compartment that cannot contain it, restriction of the muscles of facial expression and stretching of the skin envelope, and the accumulated payload of every previous session. It is not simply a matter of taste or of one bad injection.
Will dissolving my filler give me my old face back?
No, and this is the most important expectation to correct. Dissolving removes the filler; it does not reverse time. The face revealed underneath is older and often looser than the face you remember, partly because years have passed and partly because skin held out by filler does not always spring back. What dissolving gives you is an accurate face to plan from.
Does hyaluronidase damage your own tissue?
It can, because it is not selective. Hyaluronidase breaks down hyaluronic acid, and your skin contains its own hyaluronic acid that has nothing to do with the filler. Aggressive or repeated use has been associated with hollowing around the eyes, worsening fine lines, and deterioration in skin quality, a pattern described as posthyaluronidase syndrome. This is a reason to dissolve deliberately and adequately once, rather than repeatedly and cautiously.
How long after dissolving filler can I have a facelift?
In my practice, about two weeks. The filler itself breaks down within one to three days, so the wait is not for the enzyme. It is for the swelling to settle and the face to reach its true resting shape, because a lift planned on a face that is still changing is a lift planned on the wrong face.
Do I have to dissolve my filler before a facelift?
If you have had significant filler, yes, and I ask for it. Dissolving makes the operation easier and safer, because filler and the fibrosis around it obscure the surgical planes, increase bleeding and therefore the risk of a hematoma, and make injury to tissue more likely. In a survey of Aesthetic Society members, 51.9 percent said a history of panfacial filler increased the difficulty of a facelift.
Why can a surgeon not just lift a face with the filler still in it?
Because you would be under-lifted without anyone realizing it. Filler props up the skin, so less skin appears redundant on the day of surgery, and less skin gets removed. When the filler eventually recedes, the skin that was being held out has nowhere to go and sags again. A face has to be lifted when its skin redundancy is at maximum, and that is after the filler is gone. Surgeons in the same survey described exactly this failure, reporting a lifting effect that did not last as long in patients with a filler history.
Will I be left hollow after the filler is dissolved?
Sometimes, and it is a fair thing to worry about. My answer is to correct the volume with fat grafted from your own body during the lift itself, rather than with more product. Fat that survives survives as living tissue and does not carry the accumulation problem that repeated filler does.
Does filler make a facelift more dangerous?
It makes it more difficult, and difficulty and risk are related. Filler is encountered in the surgical planes, the tissue around it is fibrotic, dissection is harder, bleeding is greater, and hematoma risk rises. Nearly 40 percent of surveyed surgeons believed a filler history raised postoperative complication rates, and 15.4 percent of them reported having encountered compromised blood supply to the flap. Those figures describe what surgeons report, not the odds for any individual patient.
Can filler be dissolved from anywhere on the face?
Hyaluronic acid filler can be dissolved wherever it is, including the lips, cheeks, tear troughs, and jawline. Under the eyes is the region most often dissolved, and also the region where filler was most often the wrong tool in the first place, which is the subject of the guide to under-eye surgery versus tear trough filler. What cannot be dissolved is a permanent or semipermanent filler, which hyaluronidase does not act on at all. Removing those is a surgical problem, not an enzymatic one, so knowing exactly what was injected into you matters enormously.
Why does my face look wider or heavier than it used to?
Most often because filler has spread beyond the compartment it was placed in, blurring the boundaries that give a face its definition, and because more of it has accumulated than anyone accounted for. A second possibility is that filler is being used to compensate for tissue that is descending, in which case the face gets progressively heavier without ever being lifted, and the heaviness is the price of avoiding the real diagnosis.
Is fat grafting better than filler?
For the right problem, it behaves better over time, because surviving fat is living tissue rather than a gel that has to be replenished. It is also more involved, it requires a procedure rather than an appointment, and the survival rate is a genuine variable rather than a marketing claim. It is not a universal replacement for filler, but for a face that is having its volume restored during a lift, it is the more honest choice.
I have had filler for years and I am happy. Should I be worried?
Not necessarily worried, but you should know what is in your face and stop assuming it resets between sessions. Ask for a record of how much has been injected and where. If your skin is still holding and your face is not blurring or getting heavier, you are the patient for whom filler is working. Simply keep counting.
What is the single question I should ask before my next syringe?
Is my face losing volume, or is it coming down? Filler answers the first question well and cannot answer the second at all. Almost every overfilled face is the result of that question never being asked.
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified medical professional before making any decisions about surgical or non-surgical procedures.